Lana Sargent, Kristin M Zimmerman, Almutairi Mohammed, Matthew J Barrett, Huma Nawaz, Kathryn Wyman-Chick, Marissa Mackiewicz, Youssef Roman, Patricia Slattum, Sally Russell, Dave L Dixon, Sarah K Lageman, Sarah Hobgood, Leroy R Thacker, Elvin T Price
{"title":"Low-Income Older Adults' Vulnerability to Anticholinergic Medication-Associated Frailty.","authors":"Lana Sargent, Kristin M Zimmerman, Almutairi Mohammed, Matthew J Barrett, Huma Nawaz, Kathryn Wyman-Chick, Marissa Mackiewicz, Youssef Roman, Patricia Slattum, Sally Russell, Dave L Dixon, Sarah K Lageman, Sarah Hobgood, Leroy R Thacker, Elvin T Price","doi":"10.1007/s40266-023-01069-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A growing body of research supports the negative impact of anticholinergic drug burden on physical frailty. However, prior research has been limited to homogeneous white European populations, and few studies have evaluated how anticholinergic burden tools compare in their measurement function and reliability with minority community-dwelling adult populations. This study investigated the association between anticholinergic drug exposure and frailty by conducting a sensitivity analysis using multiple anticholinergic burden tools in a diverse cohort.</p><p><strong>Methods: </strong>A comprehensive psychometric approach was used to assess the performance of five clinical Anticholinergic Burden Tools: Anticholinergic Cognitive Burden Scale (ACB), Anticholinergic Drug Scale (ADS), average daily dose, total standardized daily doses (TSDD), and Cumulative Anticholinergic Burden scale (CAB). Spearman correlation matrix and intraclass correlation coefficients (ICC) were used to determine the association among the variables. Ordinal logistic regression is used to evaluate the anticholinergic burden measured by each scale to determine the prediction of frailty. Model performance is determined by the area under the curve (AUC).</p><p><strong>Results: </strong>The cohort included 80 individuals (mean age 69 years; 55.7% female, 71% African American). All anticholinergic burden tools were highly correlated (p < 0.001), ICC3 0.66 (p < 0.001, 95% confidence interval (CI) 0.53-0.73). Among individuals prescribed anticholinergics, 33% were robust, 44% were prefrail, and 23% were frail. All five tools predicted prefrail and frail status (p < 0.05) with low model misclassification rates for frail individuals (AUC range 0.78-0.85).</p><p><strong>Conclusion: </strong>Anticholinergic burden tools evaluated in this cohort of low-income African American older adults were highly correlated and predicted prefrail and frail status. Findings indicate that clinicians can select the appropriate instrument for the clinic setting and research question while maintaining confidence that all five tools will produce reliable results. Future anticholinergic research is needed to unravel the association between interventions such as deprescribing on incident frailty in longitudinal data.</p>","PeriodicalId":11489,"journal":{"name":"Drugs & Aging","volume":" ","pages":"1123-1131"},"PeriodicalIF":3.8000,"publicationDate":"2023-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drugs & Aging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40266-023-01069-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/19 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: A growing body of research supports the negative impact of anticholinergic drug burden on physical frailty. However, prior research has been limited to homogeneous white European populations, and few studies have evaluated how anticholinergic burden tools compare in their measurement function and reliability with minority community-dwelling adult populations. This study investigated the association between anticholinergic drug exposure and frailty by conducting a sensitivity analysis using multiple anticholinergic burden tools in a diverse cohort.
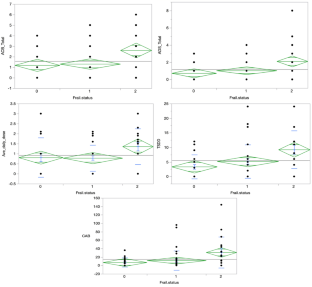
Methods: A comprehensive psychometric approach was used to assess the performance of five clinical Anticholinergic Burden Tools: Anticholinergic Cognitive Burden Scale (ACB), Anticholinergic Drug Scale (ADS), average daily dose, total standardized daily doses (TSDD), and Cumulative Anticholinergic Burden scale (CAB). Spearman correlation matrix and intraclass correlation coefficients (ICC) were used to determine the association among the variables. Ordinal logistic regression is used to evaluate the anticholinergic burden measured by each scale to determine the prediction of frailty. Model performance is determined by the area under the curve (AUC).
Results: The cohort included 80 individuals (mean age 69 years; 55.7% female, 71% African American). All anticholinergic burden tools were highly correlated (p < 0.001), ICC3 0.66 (p < 0.001, 95% confidence interval (CI) 0.53-0.73). Among individuals prescribed anticholinergics, 33% were robust, 44% were prefrail, and 23% were frail. All five tools predicted prefrail and frail status (p < 0.05) with low model misclassification rates for frail individuals (AUC range 0.78-0.85).
Conclusion: Anticholinergic burden tools evaluated in this cohort of low-income African American older adults were highly correlated and predicted prefrail and frail status. Findings indicate that clinicians can select the appropriate instrument for the clinic setting and research question while maintaining confidence that all five tools will produce reliable results. Future anticholinergic research is needed to unravel the association between interventions such as deprescribing on incident frailty in longitudinal data.
期刊介绍:
Drugs & Aging delivers essential information on the most important aspects of drug therapy to professionals involved in the care of the elderly.
The journal addresses in a timely way the major issues relating to drug therapy in older adults including: the management of specific diseases, particularly those associated with aging, age-related physiological changes impacting drug therapy, drug utilization and prescribing in the elderly, polypharmacy and drug interactions.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
