Hoang Nhat Pham, Enkhtsogt Sainbayar, Ramzi Ibrahim, Justin Z Lee
{"title":"Intracerebral hemorrhage mortality in individuals with atrial fibrillation: a nationwide analysis of mortality trends in the United States.","authors":"Hoang Nhat Pham, Enkhtsogt Sainbayar, Ramzi Ibrahim, Justin Z Lee","doi":"10.1007/s10840-023-01674-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Atrial fibrillation (AF) is a risk factor for intracerebral hemorrhage (ICH), both with and without use of anticoagulation. Limited data exists on mortality trends and disparities related to this phenomenon. We aimed to assess ICH mortality trends and disparities based on demographic factors in individuals with atrial fibrillation in the United States (US).</p><p><strong>Methods: </strong>Our cross-sectional analysis utilized mortality data from the CDC database through death certificate queries from the years 1999 to 2020 in the US. We queried for all deaths with ICH as the underlying cause of death and atrial fibrillation as the multiple causes of death. Mortality data was obtained for overall population and demographic subpopulations based on sex, race and ethnicity, and geographic region. Trend analysis and average annual-mortality percentage change (AAPC) were completed using log-linear regression models.</p><p><strong>Results: </strong>ICH age-adjusted mortality rate (AAMR) in patients with AF increased from 0.27 (95% CI 0.25-0.29) in 1999 to 0.30 (95% CI 0.29-0.32) in 2020. A higher mortality rate was observed in males (AAMR 0.33) than in females (AAMR 0.26). The highest mortality was found in Asian/Pacific Islander (AAMR: 0.32) populations, followed by White (AAMR: 0.30), Black (AAMR: 0.15), and American Indian/Alaska Native (AAMR: 0.11) populations. Southern (AAPC: 1.3%) and non-metropolitan US regions (AAPC: + 1.9%) had the highest increase in annual mortality change.</p><p><strong>Conclusion: </strong>Our findings highlight the disparities in ICH mortality in patients with AF. Further investigation is warranted to confirm these findings and evaluate for contributors to the observed disparities.</p>","PeriodicalId":16202,"journal":{"name":"Journal of Interventional Cardiac Electrophysiology","volume":" ","pages":"1117-1125"},"PeriodicalIF":2.6000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Cardiac Electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10840-023-01674-x","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/20 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Atrial fibrillation (AF) is a risk factor for intracerebral hemorrhage (ICH), both with and without use of anticoagulation. Limited data exists on mortality trends and disparities related to this phenomenon. We aimed to assess ICH mortality trends and disparities based on demographic factors in individuals with atrial fibrillation in the United States (US).
Methods: Our cross-sectional analysis utilized mortality data from the CDC database through death certificate queries from the years 1999 to 2020 in the US. We queried for all deaths with ICH as the underlying cause of death and atrial fibrillation as the multiple causes of death. Mortality data was obtained for overall population and demographic subpopulations based on sex, race and ethnicity, and geographic region. Trend analysis and average annual-mortality percentage change (AAPC) were completed using log-linear regression models.
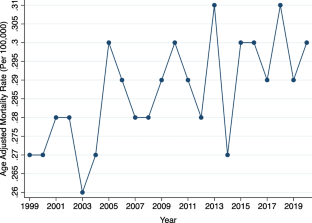
Results: ICH age-adjusted mortality rate (AAMR) in patients with AF increased from 0.27 (95% CI 0.25-0.29) in 1999 to 0.30 (95% CI 0.29-0.32) in 2020. A higher mortality rate was observed in males (AAMR 0.33) than in females (AAMR 0.26). The highest mortality was found in Asian/Pacific Islander (AAMR: 0.32) populations, followed by White (AAMR: 0.30), Black (AAMR: 0.15), and American Indian/Alaska Native (AAMR: 0.11) populations. Southern (AAPC: 1.3%) and non-metropolitan US regions (AAPC: + 1.9%) had the highest increase in annual mortality change.
Conclusion: Our findings highlight the disparities in ICH mortality in patients with AF. Further investigation is warranted to confirm these findings and evaluate for contributors to the observed disparities.
期刊介绍:
The Journal of Interventional Cardiac Electrophysiology is an international publication devoted to fostering research in and development of interventional techniques and therapies for the management of cardiac arrhythmias. It is designed primarily to present original research studies and scholarly scientific reviews of basic and applied science and clinical research in this field. The Journal will adopt a multidisciplinary approach to link physical, experimental, and clinical sciences as applied to the development of and practice in interventional electrophysiology. The Journal will examine techniques ranging from molecular, chemical and pharmacologic therapies to device and ablation technology. Accordingly, original research in clinical, epidemiologic and basic science arenas will be considered for publication. Applied engineering or physical science studies pertaining to interventional electrophysiology will be encouraged. The Journal is committed to providing comprehensive and detailed treatment of major interventional therapies and innovative techniques in a structured and clinically relevant manner. It is directed at clinical practitioners and investigators in the rapidly growing field of interventional electrophysiology. The editorial staff and board reflect this bias and include noted international experts in this area with a wealth of expertise in basic and clinical investigation. Peer review of all submissions, conflict of interest guidelines and periodic editorial board review of all Journal policies have been established.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
