Optimizing Dynamic Antibiotic Treatment Strategies against Invasive Methicillin-Resistant Staphylococcus Aureus Infections using Causal Survival Forests and G-Formula on Statewide Electronic Health Record Data.
Inyoung Jun, Scott A Cohen, Sarah E Ser, Simone Marini, Robert J Lucero, Jiang Bian, Mattia Prosperi
{"title":"Optimizing Dynamic Antibiotic Treatment Strategies against Invasive Methicillin-Resistant <i>Staphylococcus Aureus</i> Infections using Causal Survival Forests and G-Formula on Statewide Electronic Health Record Data.","authors":"Inyoung Jun, Scott A Cohen, Sarah E Ser, Simone Marini, Robert J Lucero, Jiang Bian, Mattia Prosperi","doi":"","DOIUrl":null,"url":null,"abstract":"<p><p>Developing models for individualized, time-varying treatment optimization from observational data with large variable spaces, e.g., electronic health records (EHR), is problematic because of inherent, complex bias that can change over time. Traditional methods such as the g-formula are robust, but must identify critical subsets of variables due to combinatorial issues. Machine learning approaches such as causal survival forests have fewer constraints and can provide fine-tuned, individualized counterfactual predictions. In this study, we aimed to optimize time-varying antibiotic treatment -identifying treatment heterogeneity and conditional treatment effects- against invasive methicillin-resistant <i>Staphylococcus Aureus</i> (MRSA) infections, using statewide EHR data collected in Florida, USA. While many previous studies focused on measuring the effects of the first empiric treatment (i.e., usually vancomycin), our study focuses on dynamic sequential treatment changes, comparing possible vancomycin switches with other antibiotics at clinically relevant time points, e.g., after obtaining a bacterial culture and susceptibility testing. Our study population included adult individuals admitted to the hospital with invasive MRSA. We collected demographic, clinical, medication, and laboratory information from the EHR for these patients. Then, we followed three sequential antibiotic choices (i.e., their empiric treatment, subsequent directed treatment, and final sustaining treatment), evaluating 30-day mortality as the outcome. We applied both causal survival forests and g-formula using different clinical intervention policies. We found that switching from vancomycin to another antibiotic improved survival probability, yet there was a benefit from initiating vancomycin compared to not using it at any time point. These findings show consistency with the empiric choice of vancomycin before confirmation of MRSA and shed light on how to manage switches on course. In conclusion, this application of causal machine learning on EHR demonstrates utility in modeling dynamic, heterogeneous treatment effects that cannot be evaluated precisely using randomized clinical trials.</p>","PeriodicalId":74504,"journal":{"name":"Proceedings of machine learning research","volume":"218 ","pages":"98-115"},"PeriodicalIF":0.0000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10584043/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Proceedings of machine learning research","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
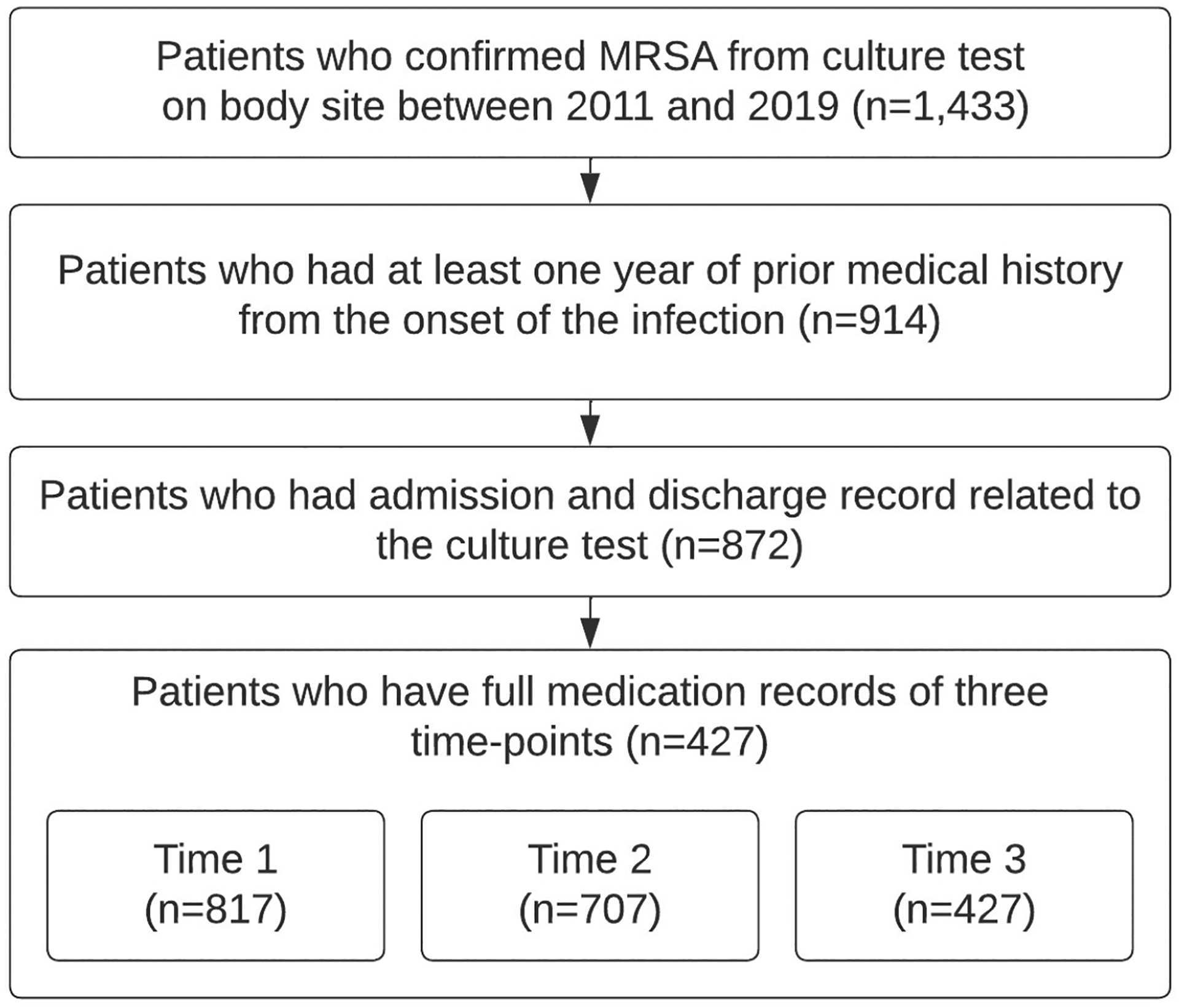
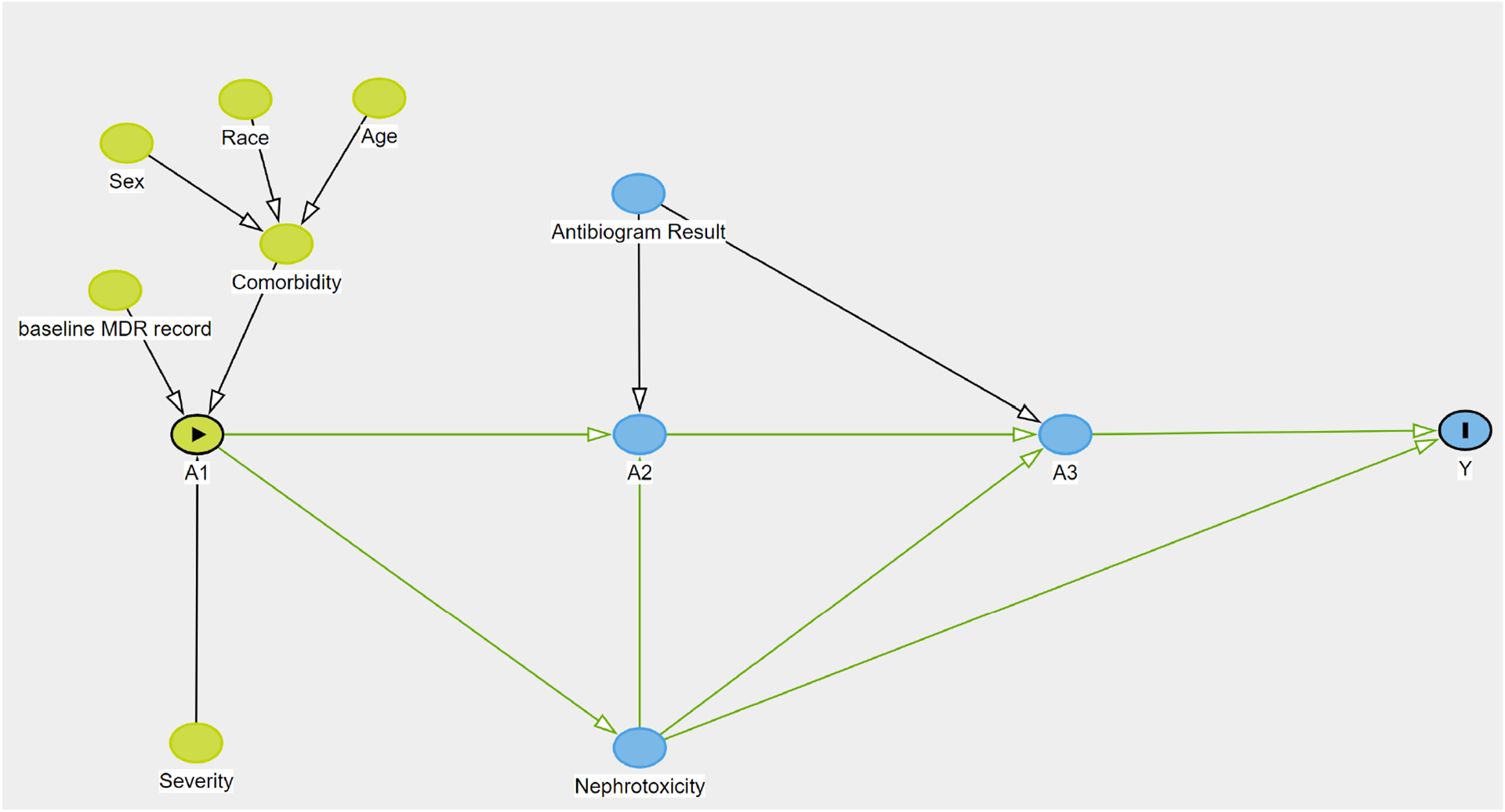
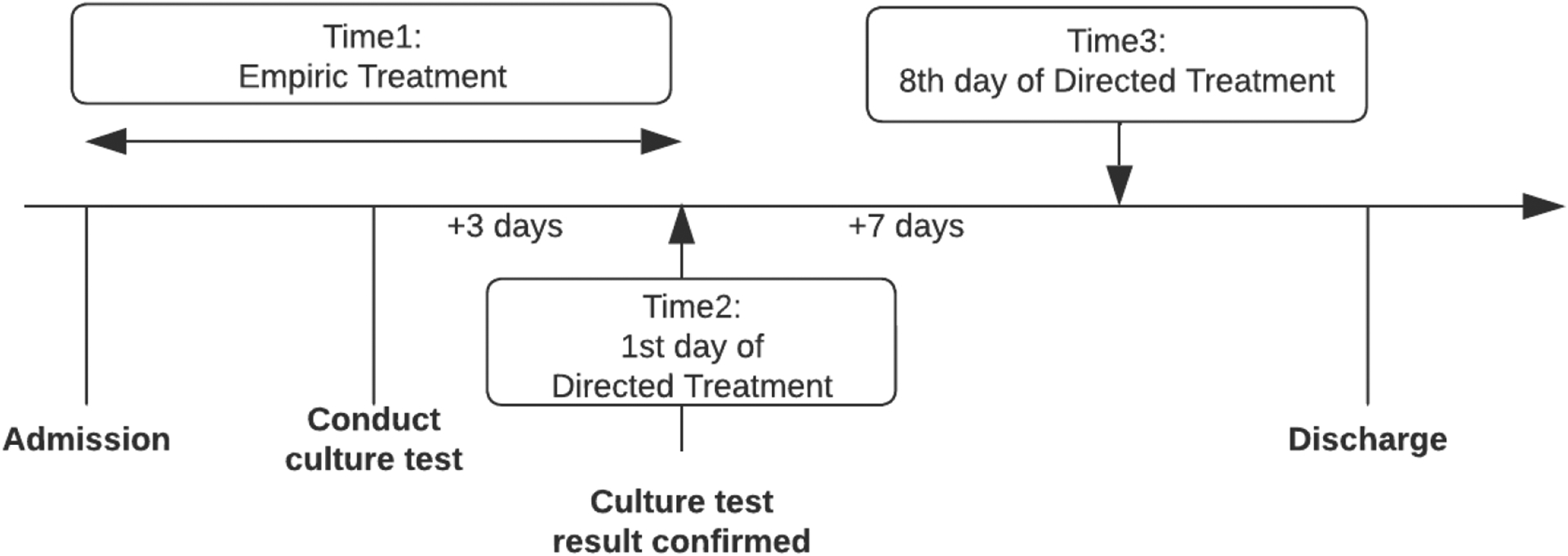
Developing models for individualized, time-varying treatment optimization from observational data with large variable spaces, e.g., electronic health records (EHR), is problematic because of inherent, complex bias that can change over time. Traditional methods such as the g-formula are robust, but must identify critical subsets of variables due to combinatorial issues. Machine learning approaches such as causal survival forests have fewer constraints and can provide fine-tuned, individualized counterfactual predictions. In this study, we aimed to optimize time-varying antibiotic treatment -identifying treatment heterogeneity and conditional treatment effects- against invasive methicillin-resistant Staphylococcus Aureus (MRSA) infections, using statewide EHR data collected in Florida, USA. While many previous studies focused on measuring the effects of the first empiric treatment (i.e., usually vancomycin), our study focuses on dynamic sequential treatment changes, comparing possible vancomycin switches with other antibiotics at clinically relevant time points, e.g., after obtaining a bacterial culture and susceptibility testing. Our study population included adult individuals admitted to the hospital with invasive MRSA. We collected demographic, clinical, medication, and laboratory information from the EHR for these patients. Then, we followed three sequential antibiotic choices (i.e., their empiric treatment, subsequent directed treatment, and final sustaining treatment), evaluating 30-day mortality as the outcome. We applied both causal survival forests and g-formula using different clinical intervention policies. We found that switching from vancomycin to another antibiotic improved survival probability, yet there was a benefit from initiating vancomycin compared to not using it at any time point. These findings show consistency with the empiric choice of vancomycin before confirmation of MRSA and shed light on how to manage switches on course. In conclusion, this application of causal machine learning on EHR demonstrates utility in modeling dynamic, heterogeneous treatment effects that cannot be evaluated precisely using randomized clinical trials.
 分享
分享



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
