Primary Total Shoulder Arthroplasty is Superior to Hemiarthroplasty for the Treatment of Glenohumeral Arthritis: Analysis of 5-year Outcomes in a Large Surgical Database.
Jason Long, Kunal Varshenya, Kier Blevins, Julia Ralph, Anna Bryniarski, Caroline Park, Lucy Meyer, Brian Lau
{"title":"Primary Total Shoulder Arthroplasty is Superior to Hemiarthroplasty for the Treatment of Glenohumeral Arthritis: Analysis of 5-year Outcomes in a Large Surgical Database.","authors":"Jason Long, Kunal Varshenya, Kier Blevins, Julia Ralph, Anna Bryniarski, Caroline Park, Lucy Meyer, Brian Lau","doi":"10.1177/24715492231207482","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Total shoulder arthroplasty (TSA) is the preferred treatment for glenohumeral arthritis refractory to nonoperative measures. However, some surgeons have argued for a role for hemiarthroplasty (HA) in the setting of a smooth glenoid that articulates appropriately with the humeral head. The purpose of this study is to evaluate long-term revision rates and short-term postoperative complications in patients undergoing either HA or TSA for glenohumeral arthritis.</p><p><strong>Methods: </strong>A retrospective review of patients who underwent HA and TSA was conducted using a commercially available national database. Demographics, postoperative complications, risk factors, revision rates, and costs were analyzed using 2 sample <i>t</i>-tests, chi-squared tests, and multivariate logistic regressions.</p><p><strong>Results: </strong>Patients were stratified by operation: (1) HA (n = 1615) or 2) TSA (n = 7845). Patients undergoing primary TSA had higher rates of prior ipsilateral rotator cuff repair and corticosteroid injections. At 2 years, patients who underwent HA, 3.0% of patients had revision surgery, compared to 1.6% of patients who underwent TSA (<i>P</i> = .002); at 5 years, 3.7% of the HA cohort (<i>P</i> < .0001) had revision surgery, compared to 1.9% of patients who underwent TSA.</p><p><strong>Conclusions: </strong>Patients undergoing TSA or RTSA for glenohumeral arthritis had higher preoperative co-morbidities but had no difference in short-term complication rates with a lower risk of revision surgery at both 2-year and 5-year follow-up when compared to HA. Increasing age, female sex, hyperlipidemia, postoperative infection, shoulder instability, and thromboembolism all independently increased odds for revision shoulder arthroplasty for glenohumeral arthritis.</p><p><strong>Level of evidence level: </strong>III.</p>","PeriodicalId":73942,"journal":{"name":"Journal of shoulder and elbow arthroplasty","volume":"7 ","pages":"24715492231207482"},"PeriodicalIF":0.0000,"publicationDate":"2023-10-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/53/03/10.1177_24715492231207482.PMC10590041.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of shoulder and elbow arthroplasty","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/24715492231207482","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Total shoulder arthroplasty (TSA) is the preferred treatment for glenohumeral arthritis refractory to nonoperative measures. However, some surgeons have argued for a role for hemiarthroplasty (HA) in the setting of a smooth glenoid that articulates appropriately with the humeral head. The purpose of this study is to evaluate long-term revision rates and short-term postoperative complications in patients undergoing either HA or TSA for glenohumeral arthritis.
Methods: A retrospective review of patients who underwent HA and TSA was conducted using a commercially available national database. Demographics, postoperative complications, risk factors, revision rates, and costs were analyzed using 2 sample t-tests, chi-squared tests, and multivariate logistic regressions.
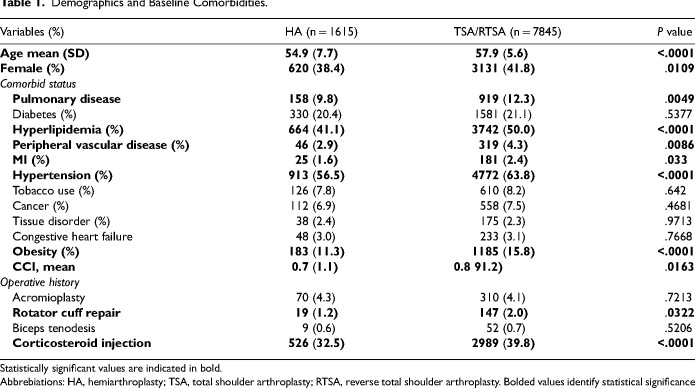
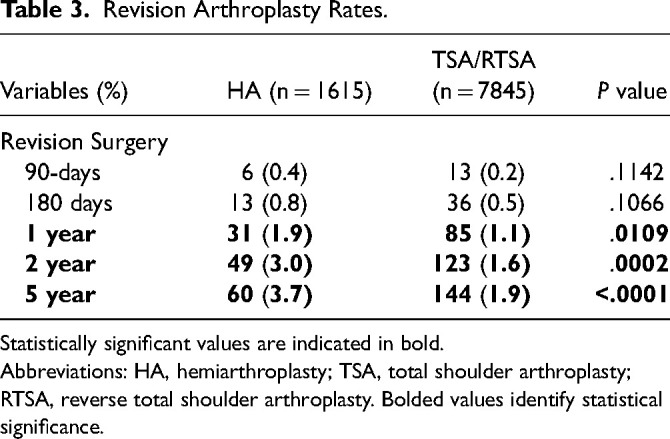
Results: Patients were stratified by operation: (1) HA (n = 1615) or 2) TSA (n = 7845). Patients undergoing primary TSA had higher rates of prior ipsilateral rotator cuff repair and corticosteroid injections. At 2 years, patients who underwent HA, 3.0% of patients had revision surgery, compared to 1.6% of patients who underwent TSA (P = .002); at 5 years, 3.7% of the HA cohort (P < .0001) had revision surgery, compared to 1.9% of patients who underwent TSA.
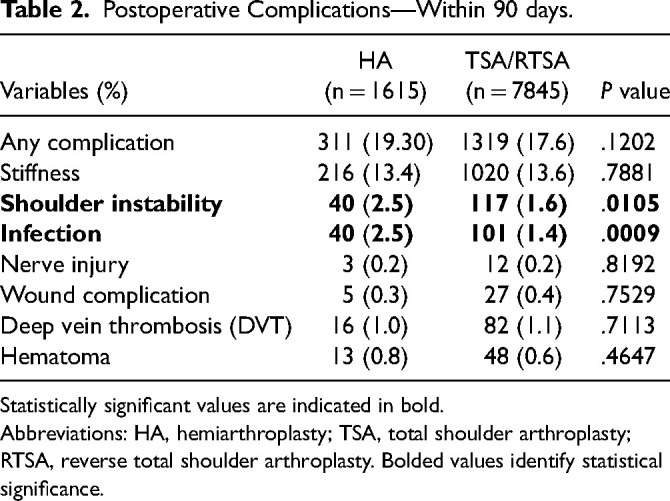
Conclusions: Patients undergoing TSA or RTSA for glenohumeral arthritis had higher preoperative co-morbidities but had no difference in short-term complication rates with a lower risk of revision surgery at both 2-year and 5-year follow-up when compared to HA. Increasing age, female sex, hyperlipidemia, postoperative infection, shoulder instability, and thromboembolism all independently increased odds for revision shoulder arthroplasty for glenohumeral arthritis.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
