Thomas Gadsden, Anushka Patel, Devarsetty Praveen, Anna Palagyi
{"title":"Transfer or tailor? Implementing a technology-supported intervention for noncommunicable diseases across contexts","authors":"Thomas Gadsden, Anushka Patel, Devarsetty Praveen, Anna Palagyi","doi":"10.1002/hcs2.26","DOIUrl":null,"url":null,"abstract":"<p>In May 2022, the 75th World Health Assembly recognized the need to accelerate national responses to the growing burden of noncommunicable diseases (NCDs) to achieve the goals of the Global Action Plan (GAP) for the Prevention and Control of NCDs. To facilitate this, an implementation roadmap was adopted that urges countries to prioritize the implementation of NCD interventions that are most appropriate to their specific local and regional context. The roadmap will act as an overarching guide for countries to tackle NCDs via three approaches: (i) Accelerate national responses based on local NCD epidemiology, risk factors and identified barriers and enablers; (ii) Prioritize and scale up the implementation of most impactful and feasible interventions according to the local context; and (iii) Ensure timely, reliable and sustained national data on NCD risk factors and mortality for data driven actions and to strengthen accountability [<span>1</span>].</p><p>With the end date of 2030 for the NCD-GAP fast approaching, the adaptation of proven interventions is likely the most efficient and effective means by which countries can make inroads into NCD control [<span>2</span>]. While investment in continued research and innovation to support such adaptation processes is vital, prior knowledge and experience with the implementation of NCD interventions highlight a series of common principles that—if leveraged—can provide programs for NCD prevention and management with the strongest chance of success. In this perspective piece we share such key principles emerging from our own experience implementing a multifaceted NCD management intervention—SMART<i>health</i> (Systematic Medical Appraisal Referral and Treatment)—across different country contexts.</p><p>SMART<i>health</i> is a technology-supported, multifaceted primary health care intervention aimed at improving the provision of guideline-based assessment and prevention or management of common NCDs. A central common component of the SMART<i>health</i> intervention is a clinical decision support system (CDSS) with context-defined variations in disease focus and approach to health system integration, including workforce strategy [<span>3</span>] (Figure 1).</p><p>The intervention was first piloted in Australia as a CDSS embedded in existing patient management information systems and delivered by general practitioners (GPs) [<span>4</span>]. Encouraged by positive outcomes (e.g., improved cardiovascular risk factor screening, namely blood pressure [BP] recording and up-titration of cardiovascular preventive drugs), the CDSS was adapted to the Indian primary health care setting by expanding the platform to include a mobile application that can be used by frontline health workers within rural communities to support early identification, referral, and management for cardiovascular disease. Though the platform was found to be acceptable by the community and health professionals across test sites in rural India, no clear evidence of clinical benefit emerged from a cluster randomized trial (e.g., no difference in achieving BP targets or receiving BP-lowering medication) [<span>5</span>, <span>6</span>]. Conversely, a subsequent trial in similar primary health care settings in rural Indonesia was strongly positive (e.g., higher use of BP-lowering medication and lower BP levels in those receiving the intervention), leading to the intervention being adopted by the local government authority for scale-up [<span>7</span>]. To further evaluate variation in implementation outcomes, pilots of the SMART<i>health</i> intervention are currently ongoing in China and Thailand [<span>8</span>].</p><p>context, health system interventions, noncommunicable diseases</p><p><b>Thomas Gadsden</b>: Writing – original draft (lead); writing – review and editing (lead). <b>Anushka Patel</b>: Conceptualization (equal); project administration (lead); writing – review and editing (equal). <b>Devarsetty Praveen</b>: Writing – review and editing (supporting). <b>Anna Palagyi</b>: Conceptualization (equal); writing – original draft (equal); writing – review and editing (equal).</p><p>The author declares no conflict of interest.</p><p>None declared.</p><p>None.</p>","PeriodicalId":100601,"journal":{"name":"Health Care Science","volume":"2 1","pages":"75-78"},"PeriodicalIF":3.3000,"publicationDate":"2022-11-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hcs2.26","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Care Science","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hcs2.26","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
In May 2022, the 75th World Health Assembly recognized the need to accelerate national responses to the growing burden of noncommunicable diseases (NCDs) to achieve the goals of the Global Action Plan (GAP) for the Prevention and Control of NCDs. To facilitate this, an implementation roadmap was adopted that urges countries to prioritize the implementation of NCD interventions that are most appropriate to their specific local and regional context. The roadmap will act as an overarching guide for countries to tackle NCDs via three approaches: (i) Accelerate national responses based on local NCD epidemiology, risk factors and identified barriers and enablers; (ii) Prioritize and scale up the implementation of most impactful and feasible interventions according to the local context; and (iii) Ensure timely, reliable and sustained national data on NCD risk factors and mortality for data driven actions and to strengthen accountability [1].
With the end date of 2030 for the NCD-GAP fast approaching, the adaptation of proven interventions is likely the most efficient and effective means by which countries can make inroads into NCD control [2]. While investment in continued research and innovation to support such adaptation processes is vital, prior knowledge and experience with the implementation of NCD interventions highlight a series of common principles that—if leveraged—can provide programs for NCD prevention and management with the strongest chance of success. In this perspective piece we share such key principles emerging from our own experience implementing a multifaceted NCD management intervention—SMARThealth (Systematic Medical Appraisal Referral and Treatment)—across different country contexts.
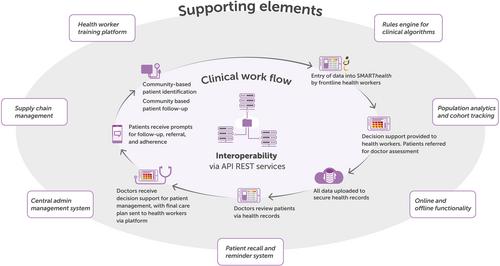
SMARThealth is a technology-supported, multifaceted primary health care intervention aimed at improving the provision of guideline-based assessment and prevention or management of common NCDs. A central common component of the SMARThealth intervention is a clinical decision support system (CDSS) with context-defined variations in disease focus and approach to health system integration, including workforce strategy [3] (Figure 1).
The intervention was first piloted in Australia as a CDSS embedded in existing patient management information systems and delivered by general practitioners (GPs) [4]. Encouraged by positive outcomes (e.g., improved cardiovascular risk factor screening, namely blood pressure [BP] recording and up-titration of cardiovascular preventive drugs), the CDSS was adapted to the Indian primary health care setting by expanding the platform to include a mobile application that can be used by frontline health workers within rural communities to support early identification, referral, and management for cardiovascular disease. Though the platform was found to be acceptable by the community and health professionals across test sites in rural India, no clear evidence of clinical benefit emerged from a cluster randomized trial (e.g., no difference in achieving BP targets or receiving BP-lowering medication) [5, 6]. Conversely, a subsequent trial in similar primary health care settings in rural Indonesia was strongly positive (e.g., higher use of BP-lowering medication and lower BP levels in those receiving the intervention), leading to the intervention being adopted by the local government authority for scale-up [7]. To further evaluate variation in implementation outcomes, pilots of the SMARThealth intervention are currently ongoing in China and Thailand [8].
context, health system interventions, noncommunicable diseases
Thomas Gadsden: Writing – original draft (lead); writing – review and editing (lead). Anushka Patel: Conceptualization (equal); project administration (lead); writing – review and editing (equal). Devarsetty Praveen: Writing – review and editing (supporting). Anna Palagyi: Conceptualization (equal); writing – original draft (equal); writing – review and editing (equal).


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
