{"title":"Pituitary macroadenoma apoplexy as a rare complication of Bruton tyrosine kinase inhibitor in chronic lymphoid leukaemia.","authors":"Aysha Gomaa, Robert Skelly","doi":"10.1186/s41016-023-00345-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pituitary apoplexy is a neurosurgical emergency and is a known yet rare complication of pituitary macroadenoma. Patients typically present with visual field defects, headache and altered sensorium. There are multiple risk factors for this complication and a thorough drug history is essential to exclude iatrogenic causes of disease. We present an extremely rare case of newly diagnosed pituitary insufficiency unveiled by ibrutinib therapy (a Bruton tyrosine kinase inhibitor). Furthermore, after initial withdrawal of ibrutinib because of the erroneous diagnosis of Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH), its re-administration led to the development of classical pituitary apoplexy 4 months after treatment was restarted.</p><p><strong>Case presentation: </strong>A male patient in his 60s with a background of chronic lymphocytic leukaemia (CLL) on ibrutinib and venetoclax presents with acute confusion and deranged electrolytes. He is found to be hyponatraemic and is diagnosed with Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) and treated with fluid restriction. He represents again 3 weeks later with hyponatraemia and further investigations reveal pituitary insufficiency and macroadenoma. He was restarted on ibrutinib and venetoclax at the time of discharge. Four months later, he presents with sudden retro-orbital headache associated with vomiting. Clinical findings include cranial nerve III, IV and XI palsy. Humphrey's visual field examination revealed a left visual field index (VFI) of only 1% while the right was 64% with temporal hemianopia. Both pupils were mid-dilated and poorly reactive to light. MRI pituitary with contrast showed features of pituitary apoplexy and optic nerve compression. He was urgently referred to the neurosurgical team and underwent an emergency trans-sphenoidal hypophysectomy with circumferential excision of the macroadenoma. Post-operative recovery was uneventful with marked improvement in vision bilaterally. The patient was restarted on ibrutinib and venetoclax 2 weeks post-operatively. Approximately 1 year post-treatment, he remains in radiological, clinical and biochemical remission from CLL and all medications have been withdrawn.</p><p><strong>Conclusions: </strong>This is a unique and rare case of pituitary macroadenoma apoplexy following the commencement of ibrutinib for CLL. Central nervous system haemorrhage is a rare side effect of ibrutinib due to its platelet dysfunction effects. A thorough assessment is required to assess the risks and benefits of using ibrutinib in patients with pituitary macroadenoma to avoid serious complications.</p>","PeriodicalId":36700,"journal":{"name":"Chinese Neurosurgical Journal","volume":"9 1","pages":"30"},"PeriodicalIF":0.0000,"publicationDate":"2023-10-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10594721/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chinese Neurosurgical Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s41016-023-00345-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Pituitary apoplexy is a neurosurgical emergency and is a known yet rare complication of pituitary macroadenoma. Patients typically present with visual field defects, headache and altered sensorium. There are multiple risk factors for this complication and a thorough drug history is essential to exclude iatrogenic causes of disease. We present an extremely rare case of newly diagnosed pituitary insufficiency unveiled by ibrutinib therapy (a Bruton tyrosine kinase inhibitor). Furthermore, after initial withdrawal of ibrutinib because of the erroneous diagnosis of Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH), its re-administration led to the development of classical pituitary apoplexy 4 months after treatment was restarted.
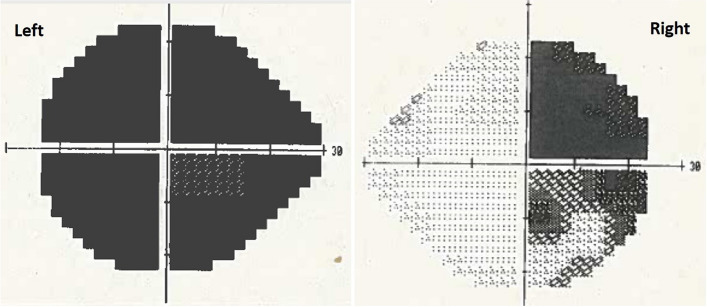
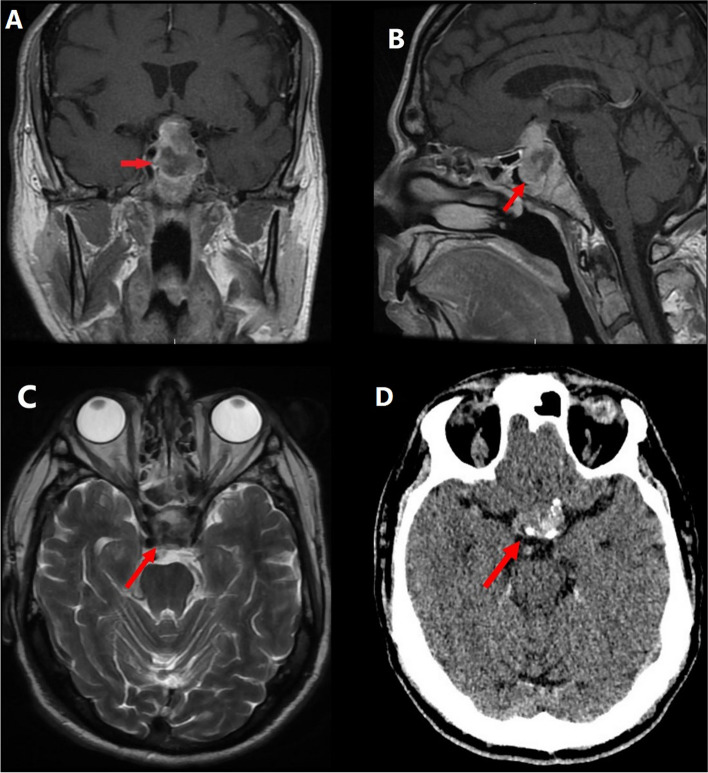
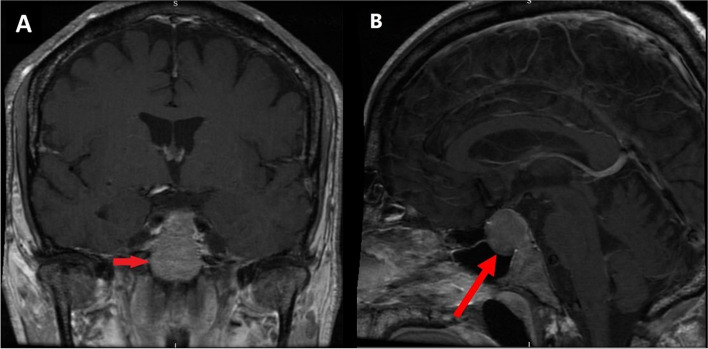
Case presentation: A male patient in his 60s with a background of chronic lymphocytic leukaemia (CLL) on ibrutinib and venetoclax presents with acute confusion and deranged electrolytes. He is found to be hyponatraemic and is diagnosed with Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) and treated with fluid restriction. He represents again 3 weeks later with hyponatraemia and further investigations reveal pituitary insufficiency and macroadenoma. He was restarted on ibrutinib and venetoclax at the time of discharge. Four months later, he presents with sudden retro-orbital headache associated with vomiting. Clinical findings include cranial nerve III, IV and XI palsy. Humphrey's visual field examination revealed a left visual field index (VFI) of only 1% while the right was 64% with temporal hemianopia. Both pupils were mid-dilated and poorly reactive to light. MRI pituitary with contrast showed features of pituitary apoplexy and optic nerve compression. He was urgently referred to the neurosurgical team and underwent an emergency trans-sphenoidal hypophysectomy with circumferential excision of the macroadenoma. Post-operative recovery was uneventful with marked improvement in vision bilaterally. The patient was restarted on ibrutinib and venetoclax 2 weeks post-operatively. Approximately 1 year post-treatment, he remains in radiological, clinical and biochemical remission from CLL and all medications have been withdrawn.
Conclusions: This is a unique and rare case of pituitary macroadenoma apoplexy following the commencement of ibrutinib for CLL. Central nervous system haemorrhage is a rare side effect of ibrutinib due to its platelet dysfunction effects. A thorough assessment is required to assess the risks and benefits of using ibrutinib in patients with pituitary macroadenoma to avoid serious complications.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
