{"title":"An uncommon cause of pancreatitis with obstructive jaundice","authors":"Chang-Shen Tseng, Ming-Wun Wong, Chien-Lin Chen","doi":"10.1002/aid2.13355","DOIUrl":null,"url":null,"abstract":"<p>A 56-year-old man with a history of diabetes mellitus poorly controlled recently (HbA1c: 7.5%, <6%) presented with a 3-month history of postprandial epigastric pain, 10-kg weight loss, steatorrhea, tea-colored urine, and clay-colored stool. Physical examination revealed yellowish skin and icteric sclera but no peripheral stigmata of cirrhosis. Laboratory investigation was significant for elevated aspartate aminotransferase (289 IU/L, 8-31 IU/L), alanine aminotransferase (613 IU/L, 0-41 IU/L), alkaline phosphatase (595 U/L, 34-104 U/L), γ-glutamyl transferase (758 U/L, 0-26 U/L), total and direct bilirubin (8.0/6.1 mg/dL, 0.3-1/0.03-0.18 mg/dL), and carbohydrate antigen 19-9 (289 U/mL, <37 U/mL). Contrast-enhanced computed tomography revealed diffuse enlargement of the pancreas (arrow) and dilatation of the common bile duct (CBD) without identifiable stone or a mass lesion (arrowhead; Figure 1A). Endoscopic ultrasound (EUS) demonstrated hyperechoic foci and strands in the enlarged pancreas (arrow) and layer-by-layer whole wall thickening with a hyper-hypo-hyperechoic series (sandwich pattern) of CBD (arrowhead) as well as gallbladder (star; Figure 1B). Magnetic resonance cholangiopancreatography (MRCP) showed dilated CBD with distal tapering near the pancreatic head (arrow; Figure 1C). The diagnosis of autoimmune pancreatitis was confirmed by serologic immunoglobulin G4 (IgG 4) elevation (IgG 4: 2880 mg/dL, 3-201 mg/dL) and favored type I according to nonductal Level 1/Level 2 criteria of international consensus diagnostic criteria.<span><sup>1</sup></span> The patient recovered from jaundice and gained weight after treatment of prednisone 40 mg/d for 4 weeks, then taper by 5 mg/wk. The 8-week follow-up EUS demonstrated normalization of pancreatic size (arrow) and CBD morphology (arrowhead; Figure 2).<span><sup>2</sup></span> Autoimmune pancreatitis mimicking pancreatic cancer is a rare cause of obstructive jaundice with an estimated incidence of 1 per 100 000.<span><sup>3</sup></span> In summary, we demonstrated a case of autoimmune pancreatitis diagnosed by complement image study and elevating serum IgG 4, which achieved successful medical treatment of obstructive jaundice without further invasive procedures.<span><sup>1</sup></span></p><p>The authors declare no conflicts of interest.</p><p>This report was approved by the Research Ethical Committee of Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation (No. CR111-08).</p>","PeriodicalId":7278,"journal":{"name":"Advances in Digestive Medicine","volume":"11 2","pages":"103-104"},"PeriodicalIF":0.4000,"publicationDate":"2022-12-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13355","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Digestive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13355","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
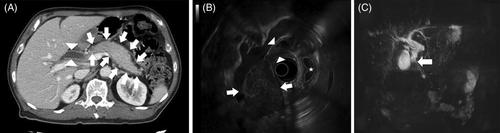
A 56-year-old man with a history of diabetes mellitus poorly controlled recently (HbA1c: 7.5%, <6%) presented with a 3-month history of postprandial epigastric pain, 10-kg weight loss, steatorrhea, tea-colored urine, and clay-colored stool. Physical examination revealed yellowish skin and icteric sclera but no peripheral stigmata of cirrhosis. Laboratory investigation was significant for elevated aspartate aminotransferase (289 IU/L, 8-31 IU/L), alanine aminotransferase (613 IU/L, 0-41 IU/L), alkaline phosphatase (595 U/L, 34-104 U/L), γ-glutamyl transferase (758 U/L, 0-26 U/L), total and direct bilirubin (8.0/6.1 mg/dL, 0.3-1/0.03-0.18 mg/dL), and carbohydrate antigen 19-9 (289 U/mL, <37 U/mL). Contrast-enhanced computed tomography revealed diffuse enlargement of the pancreas (arrow) and dilatation of the common bile duct (CBD) without identifiable stone or a mass lesion (arrowhead; Figure 1A). Endoscopic ultrasound (EUS) demonstrated hyperechoic foci and strands in the enlarged pancreas (arrow) and layer-by-layer whole wall thickening with a hyper-hypo-hyperechoic series (sandwich pattern) of CBD (arrowhead) as well as gallbladder (star; Figure 1B). Magnetic resonance cholangiopancreatography (MRCP) showed dilated CBD with distal tapering near the pancreatic head (arrow; Figure 1C). The diagnosis of autoimmune pancreatitis was confirmed by serologic immunoglobulin G4 (IgG 4) elevation (IgG 4: 2880 mg/dL, 3-201 mg/dL) and favored type I according to nonductal Level 1/Level 2 criteria of international consensus diagnostic criteria.1 The patient recovered from jaundice and gained weight after treatment of prednisone 40 mg/d for 4 weeks, then taper by 5 mg/wk. The 8-week follow-up EUS demonstrated normalization of pancreatic size (arrow) and CBD morphology (arrowhead; Figure 2).2 Autoimmune pancreatitis mimicking pancreatic cancer is a rare cause of obstructive jaundice with an estimated incidence of 1 per 100 000.3 In summary, we demonstrated a case of autoimmune pancreatitis diagnosed by complement image study and elevating serum IgG 4, which achieved successful medical treatment of obstructive jaundice without further invasive procedures.1
The authors declare no conflicts of interest.
This report was approved by the Research Ethical Committee of Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation (No. CR111-08).
期刊介绍:
Advances in Digestive Medicine is the official peer-reviewed journal of GEST, DEST and TASL. Missions of AIDM are to enhance the quality of patient care, to promote researches in gastroenterology, endoscopy and hepatology related fields, and to develop platforms for digestive science. Specific areas of interest are included, but not limited to: • Acid-related disease • Small intestinal disease • Digestive cancer • Diagnostic & therapeutic endoscopy • Enteral nutrition • Innovation in endoscopic technology • Functional GI • Hepatitis • GI images • Liver cirrhosis • Gut hormone • NASH • Helicobacter pylori • Cancer screening • IBD • Laparoscopic surgery • Infectious disease of digestive tract • Genetics and metabolic disorder • Microbiota • Regenerative medicine • Pancreaticobiliary disease • Guideline & consensus.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
