The implications when offering percutaneous nephrostomy for the management of malignant obstructive uropathy secondary to urological malignancy: can we be more selective?
Elizabeth Osinibi, Hong Doan, Alejandro Mercado-Campero, Jayasimha Abbaraju, Shikohe Masood, Sanjeev Madaan
{"title":"The implications when offering percutaneous nephrostomy for the management of malignant obstructive uropathy secondary to urological malignancy: can we be more selective?","authors":"Elizabeth Osinibi, Hong Doan, Alejandro Mercado-Campero, Jayasimha Abbaraju, Shikohe Masood, Sanjeev Madaan","doi":"10.1177/17562872231207729","DOIUrl":null,"url":null,"abstract":"Background & Objectives: Percutaneous nephrostomy (PN) for malignant ureteric obstruction (MUO) is increasingly accessible with high success rates. However, it is not without associated risks and morbidity, impacting quality of life, while not improving overall survival. In two UK hospitals, we investigated the outcomes of undergoing PN for MUO, to inform future patient counselling and selection for this intervention. Methods: A retrospective audit of electronic records identified patients that received PN for bladder, and prostate cancer (PCa) between January 2015 and December 2018. Hospital 1 had a 24-h nephrostomy service, while Hospital 2 had a limited service; Group A: recurrent or treatment-resistant PCa, Group B: primary PCa, Group C: Bladder cancer. Results: A total of 261 patients (Hospital 1 = 186, Hospital 2 = 75), had PN insertion. Seventy-eight had prostate or bladder cancer. Group A n = 30, Group B n = 12, Group C n = 36. Median age = 79 [interquartile range (IQR) = 72–86]. Following PN insertion, 12-month mortality was significantly greater in Hospital 1 at 82%, versus 52% in Hospital 2 (p = 0.015). Median survival: Group A: 177 days (IQR = 80–266), Group B: 209 days (IQR = 77–352), Group C: 145 days (IQR = 97–362). There was no significant difference in same-admission mortality, although group A had the greatest same-admission mortality at 17%. A total of 69% of all patients received bilateral nephrostomies. Patients with bilateral versus unilateral PN had no difference in mortality or nadir creatinine. Conclusion: Most patients with malignant obstruction secondary to prostate or bladder cancer lived less than 12 months after PN insertion. When offering PN, careful consideration of disease prognosis should be made, and frank discussion of the implications of a life-long nephrostomy with patients and relatives.","PeriodicalId":23010,"journal":{"name":"Therapeutic Advances in Urology","volume":"15 ","pages":"17562872231207729"},"PeriodicalIF":3.5000,"publicationDate":"2023-10-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10612453/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Urology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562872231207729","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
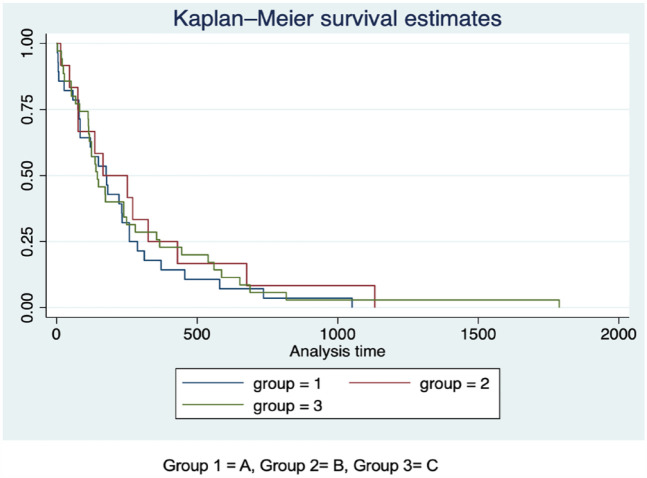
Background & Objectives: Percutaneous nephrostomy (PN) for malignant ureteric obstruction (MUO) is increasingly accessible with high success rates. However, it is not without associated risks and morbidity, impacting quality of life, while not improving overall survival. In two UK hospitals, we investigated the outcomes of undergoing PN for MUO, to inform future patient counselling and selection for this intervention. Methods: A retrospective audit of electronic records identified patients that received PN for bladder, and prostate cancer (PCa) between January 2015 and December 2018. Hospital 1 had a 24-h nephrostomy service, while Hospital 2 had a limited service; Group A: recurrent or treatment-resistant PCa, Group B: primary PCa, Group C: Bladder cancer. Results: A total of 261 patients (Hospital 1 = 186, Hospital 2 = 75), had PN insertion. Seventy-eight had prostate or bladder cancer. Group A n = 30, Group B n = 12, Group C n = 36. Median age = 79 [interquartile range (IQR) = 72–86]. Following PN insertion, 12-month mortality was significantly greater in Hospital 1 at 82%, versus 52% in Hospital 2 (p = 0.015). Median survival: Group A: 177 days (IQR = 80–266), Group B: 209 days (IQR = 77–352), Group C: 145 days (IQR = 97–362). There was no significant difference in same-admission mortality, although group A had the greatest same-admission mortality at 17%. A total of 69% of all patients received bilateral nephrostomies. Patients with bilateral versus unilateral PN had no difference in mortality or nadir creatinine. Conclusion: Most patients with malignant obstruction secondary to prostate or bladder cancer lived less than 12 months after PN insertion. When offering PN, careful consideration of disease prognosis should be made, and frank discussion of the implications of a life-long nephrostomy with patients and relatives.
期刊介绍:
Therapeutic Advances in Urology delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of urology.
The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in urology, providing a forum in print and online for publishing the highest quality articles in this area. The editors welcome articles of current interest across all areas of urology, including treatment of urological disorders, with a focus on emerging pharmacological therapies.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
