Mehmet Uludag, Mehmet Taner Unlu, Mehmet Kostek, Nurcihan Aygun, Ozan Caliskan, Alper Ozel, Adnan Isgor
{"title":"Management of Thyroid Nodules.","authors":"Mehmet Uludag, Mehmet Taner Unlu, Mehmet Kostek, Nurcihan Aygun, Ozan Caliskan, Alper Ozel, Adnan Isgor","doi":"10.14744/SEMB.2023.06992","DOIUrl":null,"url":null,"abstract":"<p><p>Thyroid nodules are common and the prevalence varies between 4 and 7% by palpation and 19-68% by high-resolution USG. Most thyroid nodules are benign, and the malignancy rate varies between 7 and 15% of patients. Thyroid nodules are detected incidentally during clinical examination or, more often, during imaging studies performed for another reason. All detected thyroid nodules should be evaluated clinically. The main test in evaluating thyroid function is thyroid stimulating hormone (TSH). If the serum TSH level is below the normal reference range, a radionuclide thyroid scan should be performed to determine whether the nodule is hyperfunctioning. If the serum TSH level is normal or high, ultrasonography (US) should be performed to evaluate the nodule. US is the most sensitive imaging method in the evaluation of thyroid nodules. Computed tomography (CT) and magnetic resonance imaging are not routinely used in the initial evaluation of thyroid nodules. There are many risk classification systems according to the USG characteristics of thyroid nodules, and the most widely used in clinical practice are the American Thyroid Association guideline and the American College of Radiology Thyroid Imaging Reporting and Data System. Fine needle aspiration biopsy (FNAB) is the gold standard method in the evaluation of nodules with indication according to USG risk class. In the cytological evaluation of FNAB, the Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) is the most frequently applied cytological classification. TBSRTC is a simplified, 6-category reporting system and was updated in 2023. The application of molecular tests to FNAB specimens, especially those diagnosed with Bethesda III and IV, is increasing to reduce the need for diagnostic surgery. Especially in Bethesda III and IV nodules, different methods are applied in the treatment of nodules according to the malignancy risk of each category, these are follow-up, surgical treatment, radioactive iodine treatment, and non-surgical ablation methods.</p>","PeriodicalId":42218,"journal":{"name":"Medical Bulletin of Sisli Etfal Hospital","volume":"57 3","pages":"287-304"},"PeriodicalIF":0.9000,"publicationDate":"2023-09-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10600596/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Bulletin of Sisli Etfal Hospital","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14744/SEMB.2023.06992","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
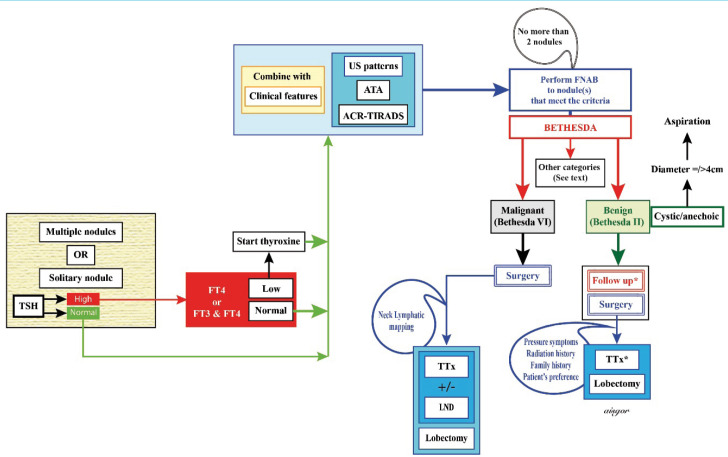
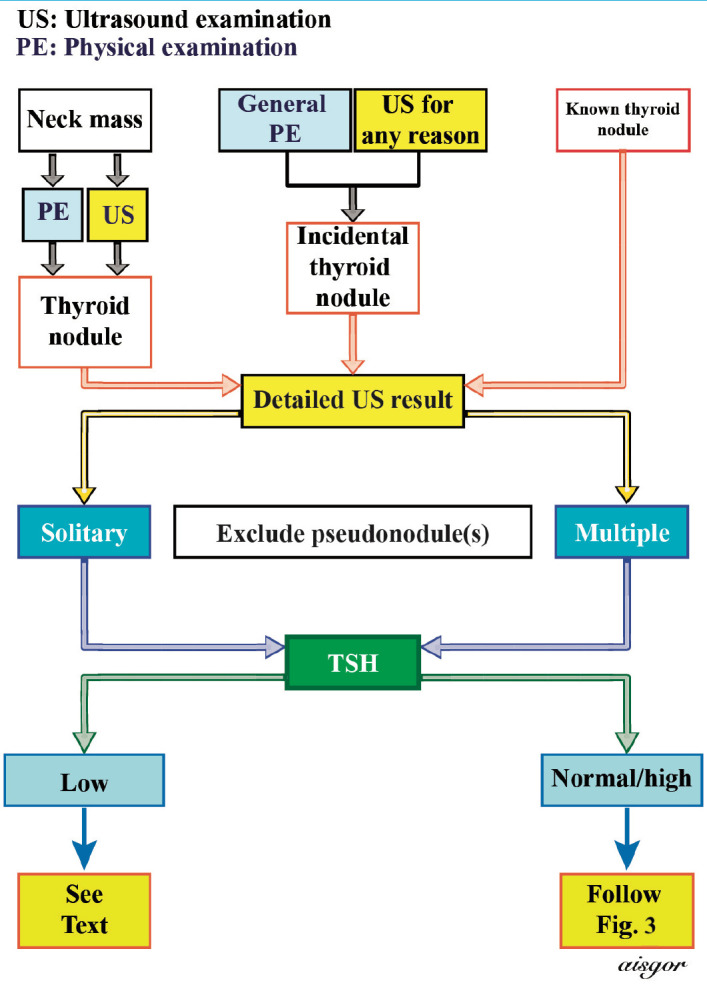
Thyroid nodules are common and the prevalence varies between 4 and 7% by palpation and 19-68% by high-resolution USG. Most thyroid nodules are benign, and the malignancy rate varies between 7 and 15% of patients. Thyroid nodules are detected incidentally during clinical examination or, more often, during imaging studies performed for another reason. All detected thyroid nodules should be evaluated clinically. The main test in evaluating thyroid function is thyroid stimulating hormone (TSH). If the serum TSH level is below the normal reference range, a radionuclide thyroid scan should be performed to determine whether the nodule is hyperfunctioning. If the serum TSH level is normal or high, ultrasonography (US) should be performed to evaluate the nodule. US is the most sensitive imaging method in the evaluation of thyroid nodules. Computed tomography (CT) and magnetic resonance imaging are not routinely used in the initial evaluation of thyroid nodules. There are many risk classification systems according to the USG characteristics of thyroid nodules, and the most widely used in clinical practice are the American Thyroid Association guideline and the American College of Radiology Thyroid Imaging Reporting and Data System. Fine needle aspiration biopsy (FNAB) is the gold standard method in the evaluation of nodules with indication according to USG risk class. In the cytological evaluation of FNAB, the Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) is the most frequently applied cytological classification. TBSRTC is a simplified, 6-category reporting system and was updated in 2023. The application of molecular tests to FNAB specimens, especially those diagnosed with Bethesda III and IV, is increasing to reduce the need for diagnostic surgery. Especially in Bethesda III and IV nodules, different methods are applied in the treatment of nodules according to the malignancy risk of each category, these are follow-up, surgical treatment, radioactive iodine treatment, and non-surgical ablation methods.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
