V. Katerenchuk, A. Calçada, A. C. Batista, L. Cordeiro
{"title":"Falsely increased Bispectral Index™ due to neuromuscular transmission monitoring","authors":"V. Katerenchuk, A. Calçada, A. C. Batista, L. Cordeiro","doi":"10.1002/anr3.12256","DOIUrl":null,"url":null,"abstract":"<p>Numerous sources of interference with Bispectral Index™ (BIS) values have been reported, including electrocautery, forced-air-warming devices, and pacemakers [<span>1-3</span>], electrical artefact can be misinterpreted by the BIS algorithm, resulting in misleading values [<span>1</span>].</p><p>Quantitative neuromuscular monitoring at the corrugator supercilii muscle is of particular utility when a patient's arms are not accessible due to surgical positioning. However, this site, involving electrodes applied to the patient's forehead, might impair BIS interpretation. We observed these changes during a steady state of general anaesthesia with a BIS Vista sensor (Covidien, Dublin, Ireland) placed on the left forehead of a patient undergoing laparoscopic abdominal surgery.</p><p>After achieving a constant effect-site concentration of propofol and an appropriate depth of anaesthesia according to BIS monitoring, and assuring neuromuscular blockade with a bolus of rocuronium, we set up a train of four (TOF) acceleromyography monitor (ToFscan®, Dräger Medical, Lübeck, Germany) with a stimulating current set at 30 mA and stimulating electrodes placed over the facial nerve, as shown in Figure 1.</p><p>Within 1 min of placing the TOF electrodes (without obtaining measurements, just with the monitor turned on), a sustained increase of between 5 and 15 points in the BIS value was observed. There were no other indications of a variation in anaesthetic depth, and there were no expected surgically induced variations in anaesthetic requirements. The BIS monitor displayed optimal signal quality (full bars), but the electromyogram (EMG) signal indicator increased slightly. Switching off the TOF monitor (maintaining connector cables applied), caused a reduction to the previously observed BIS values within 2 min.</p><p>This unexpected increase in BIS value may be explained by the fact that TOF electrode connector cables, simply attached with the monitor turned on, are a source of electrical noise [<span>1, 3, 4</span>]. When asked about potential interference, the manufacturer of ToFscan suggested that a probable explanation is related to frequent and periodic (every few seconds) impedance checks. Additionally, in accordance with our observations, they reported that this interference is not present when the stimulating electrodes are placed over the ulnar nerve and is no greater than that of an electric scalpel. With that in mind, using a standard digital multimeter, we measured the voltage between the two TOF electrodes and verified repeating brief rises to a maximum of 27 mV (a typical adult human electroencephalogram signal is up to 200 μV), which supports the previous explanation.</p><p>When BIS values are exceedingly high and inconsistent with clinical assessment, one should carefully confirm that no sources of interference are present. Subtle changes may go unnoticed by the BIS signal quality indicator [<span>1</span>]. Although variation in-between the boundaries of the target range of 40 to 60 may be of small clinical importance, increases over 60, particularly in frail patients, could potentially lead to harmful effects associated with unnecessary deepening of the hypnotic state [<span>5</span>].</p><p>When assessing TOF count at the corrugator supercilii muscle, the BIS value can be falsely elevated, and one possible solution is to turn off the TOF between readings and avoid timed automatic measurements.</p>","PeriodicalId":72186,"journal":{"name":"Anaesthesia reports","volume":"11 2","pages":""},"PeriodicalIF":0.8000,"publicationDate":"2023-10-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10609538/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anaesthesia reports","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/anr3.12256","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Numerous sources of interference with Bispectral Index™ (BIS) values have been reported, including electrocautery, forced-air-warming devices, and pacemakers [1-3], electrical artefact can be misinterpreted by the BIS algorithm, resulting in misleading values [1].
Quantitative neuromuscular monitoring at the corrugator supercilii muscle is of particular utility when a patient's arms are not accessible due to surgical positioning. However, this site, involving electrodes applied to the patient's forehead, might impair BIS interpretation. We observed these changes during a steady state of general anaesthesia with a BIS Vista sensor (Covidien, Dublin, Ireland) placed on the left forehead of a patient undergoing laparoscopic abdominal surgery.
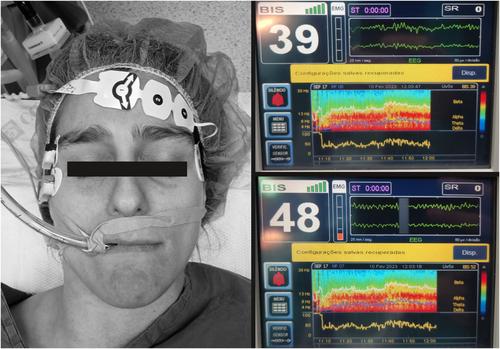
After achieving a constant effect-site concentration of propofol and an appropriate depth of anaesthesia according to BIS monitoring, and assuring neuromuscular blockade with a bolus of rocuronium, we set up a train of four (TOF) acceleromyography monitor (ToFscan®, Dräger Medical, Lübeck, Germany) with a stimulating current set at 30 mA and stimulating electrodes placed over the facial nerve, as shown in Figure 1.
Within 1 min of placing the TOF electrodes (without obtaining measurements, just with the monitor turned on), a sustained increase of between 5 and 15 points in the BIS value was observed. There were no other indications of a variation in anaesthetic depth, and there were no expected surgically induced variations in anaesthetic requirements. The BIS monitor displayed optimal signal quality (full bars), but the electromyogram (EMG) signal indicator increased slightly. Switching off the TOF monitor (maintaining connector cables applied), caused a reduction to the previously observed BIS values within 2 min.
This unexpected increase in BIS value may be explained by the fact that TOF electrode connector cables, simply attached with the monitor turned on, are a source of electrical noise [1, 3, 4]. When asked about potential interference, the manufacturer of ToFscan suggested that a probable explanation is related to frequent and periodic (every few seconds) impedance checks. Additionally, in accordance with our observations, they reported that this interference is not present when the stimulating electrodes are placed over the ulnar nerve and is no greater than that of an electric scalpel. With that in mind, using a standard digital multimeter, we measured the voltage between the two TOF electrodes and verified repeating brief rises to a maximum of 27 mV (a typical adult human electroencephalogram signal is up to 200 μV), which supports the previous explanation.
When BIS values are exceedingly high and inconsistent with clinical assessment, one should carefully confirm that no sources of interference are present. Subtle changes may go unnoticed by the BIS signal quality indicator [1]. Although variation in-between the boundaries of the target range of 40 to 60 may be of small clinical importance, increases over 60, particularly in frail patients, could potentially lead to harmful effects associated with unnecessary deepening of the hypnotic state [5].
When assessing TOF count at the corrugator supercilii muscle, the BIS value can be falsely elevated, and one possible solution is to turn off the TOF between readings and avoid timed automatic measurements.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
