Use of near infrared spectroscopy for the prediction of perioperative complications in patients undergoing elective microsurgical resection of cerebral arteriovenous malformations- a prospective observational trial (NIRSCAM trial).
{"title":"Use of near infrared spectroscopy for the prediction of perioperative complications in patients undergoing elective microsurgical resection of cerebral arteriovenous malformations- a prospective observational trial (NIRSCAM trial).","authors":"Jithumol Thankam Thomas, Ajay Prasad Hrishi P, Ranganatha Praveen, Manikandan Sethuraman, Unnikrishnan Prathapadas, Smita Vimala, Oommen Mathew","doi":"10.1007/s10877-023-01084-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Cerebral arteriovenous malformations (AVM) represent focal abnormal areas of low resistance circulation which render the peri-nidal neuronal tissue susceptible to ischemia. The post-excision cerebral perfusion surge can result in hyperaemic complications.We hypothesised that Near Infrared Spectroscopy (NIRS)-guided perioperative management can aid in the prediction and prevention of perioperative complications in patients presenting for surgical excision of cerebral AVMs. We also intended to identify a threshold value of regional cerebral oxygen saturation (rScO<sub>2</sub>) to predict the incidence of perioperative complications.</p><p><strong>Methods: </strong>This was a prospective observational study involving patients undergoing elective supratentorial AVM resection surgeries. Intraoperative rScO<sub>2</sub> and hemodynamic monitoring were done and continued for postoperatively for 12 h. Any drift in rScO<sub>2</sub> by > 12% from baseline was managed as per study protocol and perioperative adverse events were recorded and analyzed. Post surgery,for analytical purpose patients were categorized into two groups, Group A - patients without complications and Group B - patients who had complications postoperatively.</p><p><strong>Results: </strong>Twenty-five patients presenting for surgical excision of cerebral AVM were recruited for this study of which 9 patients had postoperative adverse events and were allocated to group B. The ipsilateral mean rScO<sub>2</sub> at the time of complication (Pc) was significantly lower in Group B than in group A [62.08 ± 9.33 vs.70.52 ± 7.17; p = 0.04]. The mean ipsilateral rScO<sub>2</sub> drift from N2- N5 (i.e., post excision) was significantly higher in Group B than in Group A [12.01 ± 2.63% vs. 4.98 ± 5.7%;p = 0.02]. Mean ipsilateral rScO<sub>2</sub> Drift ratio (N5 :N2) was significantly higher in group B as compared to group A [1.32 ± 0.01 vs. 1.01 ± 0.06;p < 0.001]. In the immediate post excision phase, the ipsilateral mean rScO<sub>2</sub> was significantly higher in Group B at the post excision time point compared to Group A [ 83.03 ± 6.08 vs. 73.52 ± 7.07;p < 0.01)]. The mean ipsilateral rScO<sub>2</sub> drift from N1-N6 (i.e., postoperatively) was significantly higher in Group B as compared to Group A [14.96 ± 0.080% vs. 6.88 ± 4.5% ; p < 0.01]. Similarly, the Mean Ipsilateral rScO<sub>2</sub> Drift ratio (N6:N1) was significantly lower in group B as compared to group A [2.17 ± 0.02 vs. 1.05 ± 0.03 ;p < 0.0001].</p><p><strong>Conclusions: </strong>In patients undergoing cerebral AVM resection, a post-resection ipsilateral rScO2 increase by > 12% with a drift ratio of > 1.3 could signify cerebral hyperemia. A postoperative ipsilateral rScO2 drift > 14.5% with a drift ratio of 2.1 from the baseline is associated with postoperative complications in our study. Further multi-centric randomized control trials are needed to support our research findings.</p>","PeriodicalId":15513,"journal":{"name":"Journal of Clinical Monitoring and Computing","volume":" ","pages":"623-630"},"PeriodicalIF":2.2000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Monitoring and Computing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10877-023-01084-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/2 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Cerebral arteriovenous malformations (AVM) represent focal abnormal areas of low resistance circulation which render the peri-nidal neuronal tissue susceptible to ischemia. The post-excision cerebral perfusion surge can result in hyperaemic complications.We hypothesised that Near Infrared Spectroscopy (NIRS)-guided perioperative management can aid in the prediction and prevention of perioperative complications in patients presenting for surgical excision of cerebral AVMs. We also intended to identify a threshold value of regional cerebral oxygen saturation (rScO2) to predict the incidence of perioperative complications.
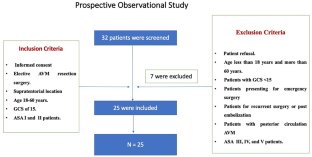
Methods: This was a prospective observational study involving patients undergoing elective supratentorial AVM resection surgeries. Intraoperative rScO2 and hemodynamic monitoring were done and continued for postoperatively for 12 h. Any drift in rScO2 by > 12% from baseline was managed as per study protocol and perioperative adverse events were recorded and analyzed. Post surgery,for analytical purpose patients were categorized into two groups, Group A - patients without complications and Group B - patients who had complications postoperatively.
Results: Twenty-five patients presenting for surgical excision of cerebral AVM were recruited for this study of which 9 patients had postoperative adverse events and were allocated to group B. The ipsilateral mean rScO2 at the time of complication (Pc) was significantly lower in Group B than in group A [62.08 ± 9.33 vs.70.52 ± 7.17; p = 0.04]. The mean ipsilateral rScO2 drift from N2- N5 (i.e., post excision) was significantly higher in Group B than in Group A [12.01 ± 2.63% vs. 4.98 ± 5.7%;p = 0.02]. Mean ipsilateral rScO2 Drift ratio (N5 :N2) was significantly higher in group B as compared to group A [1.32 ± 0.01 vs. 1.01 ± 0.06;p < 0.001]. In the immediate post excision phase, the ipsilateral mean rScO2 was significantly higher in Group B at the post excision time point compared to Group A [ 83.03 ± 6.08 vs. 73.52 ± 7.07;p < 0.01)]. The mean ipsilateral rScO2 drift from N1-N6 (i.e., postoperatively) was significantly higher in Group B as compared to Group A [14.96 ± 0.080% vs. 6.88 ± 4.5% ; p < 0.01]. Similarly, the Mean Ipsilateral rScO2 Drift ratio (N6:N1) was significantly lower in group B as compared to group A [2.17 ± 0.02 vs. 1.05 ± 0.03 ;p < 0.0001].
Conclusions: In patients undergoing cerebral AVM resection, a post-resection ipsilateral rScO2 increase by > 12% with a drift ratio of > 1.3 could signify cerebral hyperemia. A postoperative ipsilateral rScO2 drift > 14.5% with a drift ratio of 2.1 from the baseline is associated with postoperative complications in our study. Further multi-centric randomized control trials are needed to support our research findings.
期刊介绍:
The Journal of Clinical Monitoring and Computing is a clinical journal publishing papers related to technology in the fields of anaesthesia, intensive care medicine, emergency medicine, and peri-operative medicine.
The journal has links with numerous specialist societies, including editorial board representatives from the European Society for Computing and Technology in Anaesthesia and Intensive Care (ESCTAIC), the Society for Technology in Anesthesia (STA), the Society for Complex Acute Illness (SCAI) and the NAVAt (NAVigating towards your Anaestheisa Targets) group.
The journal publishes original papers, narrative and systematic reviews, technological notes, letters to the editor, editorial or commentary papers, and policy statements or guidelines from national or international societies. The journal encourages debate on published papers and technology, including letters commenting on previous publications or technological concerns. The journal occasionally publishes special issues with technological or clinical themes, or reports and abstracts from scientificmeetings. Special issues proposals should be sent to the Editor-in-Chief. Specific details of types of papers, and the clinical and technological content of papers considered within scope can be found in instructions for authors.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
