Very long-term efficacy and safety of paclitaxel-eluting balloon after a bare-metal stent for the treatment of ST-elevation myocardial infarction: 8-year results of a randomized clinical trial (PEBSI study).
Arturo García-Touchard, Manel Sabaté, Nieves Gonzalo, Vicente Peral, Beatriz Vaquerizo, Rafael Ruiz-Salmerón, Bruno García Del Blanco, Jesús Jiménez-Mazuecos, Eduardo Molina, Pedro Martínez-Romero, José María Hernandez-García, Valeriano Ruiz-Quevedo, Cristóbal Urbano, Javier Fernández-Portales, José Ramón Rumoroso, Juan Casanova-Sandoval, Eduardo Pinar, Javier Lopez-Pais, Juan Francisco Oteo, Fernando Alfonso
{"title":"Very long-term efficacy and safety of paclitaxel-eluting balloon after a bare-metal stent for the treatment of ST-elevation myocardial infarction: 8-year results of a randomized clinical trial (PEBSI study).","authors":"Arturo García-Touchard, Manel Sabaté, Nieves Gonzalo, Vicente Peral, Beatriz Vaquerizo, Rafael Ruiz-Salmerón, Bruno García Del Blanco, Jesús Jiménez-Mazuecos, Eduardo Molina, Pedro Martínez-Romero, José María Hernandez-García, Valeriano Ruiz-Quevedo, Cristóbal Urbano, Javier Fernández-Portales, José Ramón Rumoroso, Juan Casanova-Sandoval, Eduardo Pinar, Javier Lopez-Pais, Juan Francisco Oteo, Fernando Alfonso","doi":"10.21037/cdt-22-623","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Drug-eluting stents (DES) are considered the therapy of choice in ST-segment elevation myocardial infarction (STEMI); however, a low persistent rate of revascularizations and stent thrombosis exist over the time. We have previously shown that a paclitaxel (PTX)-drug-coated balloon (DCB) after a bare-metal stent (BMS) implantation (DCB-combined strategy) yields superior angiographic and clinical results compared to BMS in the short term. However, the long-term safety and efficacy of this approach remain uncertain.</p><p><strong>Methods: </strong>An 8-year clinical follow-up was conducted on patients enrolled in the randomized PEBSI-1 trial (NCT01839890). The original trial included patients who suffered a STEMI, patients were randomly assigned to receive a DCB-combined strategy or BMS only and the primary endpoint was in-stent late luminal loss (LLL) at 9-month follow-up. After the completion of this study, death, myocardial re-infarction, ischemia-driven repeated revascularizations included target lesion revascularization (TLR) and target vessel revascularization (TVR), and stent thrombosis, were assessed by yearly contact by a clinical visit, telephone or by electronic records. These outcomes were adhered to ARC-2 criteria.</p><p><strong>Results: </strong>The rate of incomplete follow-up was very low, with only 3 out of 111 patients (2.7%) in the DCB-combined strategy group and 1 out of 112 patients (0.9%) in the BMS group. At 8 years there were a lower rate of TVR [3.7% <i>vs.</i> 14.3%; hazard ratio (HR): 0.243; 95% confidence interval (CI): 0.081-0.727; P=0.006], and a trend towards lower TLR (2.8% <i>vs.</i> 8.9%; HR: 0.300; 95% CI: 0.083-1.090; P=0.052) in the DCB-combined strategy group. No statistical difference between the DCB-combined strategy and BMS groups were found for all causes of death, deaths from cardiovascular disease, reinfarctions or stent thrombosis. Notably in the DCB-combined strategy group, no episode of stent thrombosis occurred after the first year. Similarly, there were no cardiovascular deaths, TVR and TLR in the DCB-combined strategy group after 5 years. In contrast, during the period from year 5 to 8, the BMS group experienced an additional cardiovascular death, as well as one case of TVR, one case of TLR, and one case of stent thrombosis.</p><p><strong>Conclusions: </strong>In STEMI patients, the DCB-combined strategy maintains its safety and clinical efficacy over time. Our rates of TVR, TLR, and very late stent thrombosis (VLST) at very long-term are the lowest ever found in a STEMI trial. Further studies are warranted to assess the potential superiority of this novel strategy as compared with new-generation DES to prevent very late events in these patients.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov; identifier: NCT01839890.</p>","PeriodicalId":9592,"journal":{"name":"Cardiovascular diagnosis and therapy","volume":"13 5","pages":"792-804"},"PeriodicalIF":2.1000,"publicationDate":"2023-10-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10628420/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular diagnosis and therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/cdt-22-623","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/17 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Drug-eluting stents (DES) are considered the therapy of choice in ST-segment elevation myocardial infarction (STEMI); however, a low persistent rate of revascularizations and stent thrombosis exist over the time. We have previously shown that a paclitaxel (PTX)-drug-coated balloon (DCB) after a bare-metal stent (BMS) implantation (DCB-combined strategy) yields superior angiographic and clinical results compared to BMS in the short term. However, the long-term safety and efficacy of this approach remain uncertain.
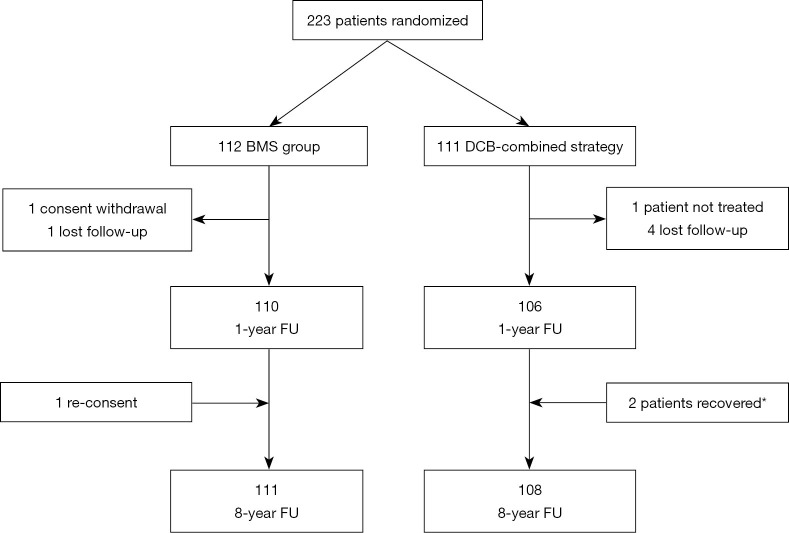
Methods: An 8-year clinical follow-up was conducted on patients enrolled in the randomized PEBSI-1 trial (NCT01839890). The original trial included patients who suffered a STEMI, patients were randomly assigned to receive a DCB-combined strategy or BMS only and the primary endpoint was in-stent late luminal loss (LLL) at 9-month follow-up. After the completion of this study, death, myocardial re-infarction, ischemia-driven repeated revascularizations included target lesion revascularization (TLR) and target vessel revascularization (TVR), and stent thrombosis, were assessed by yearly contact by a clinical visit, telephone or by electronic records. These outcomes were adhered to ARC-2 criteria.
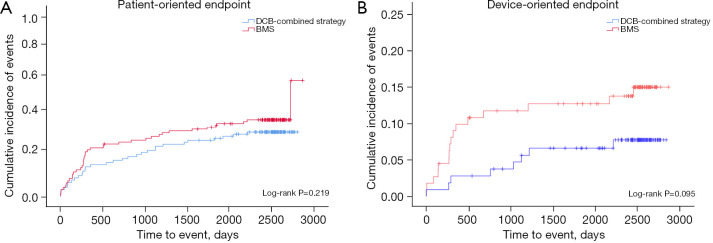
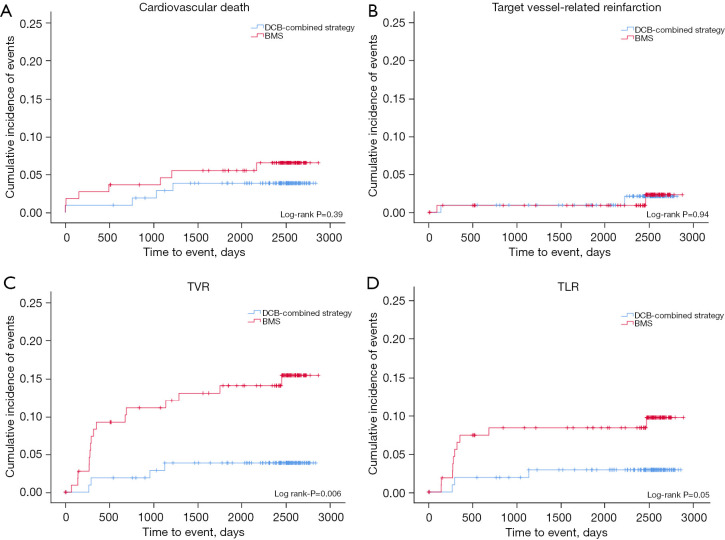
Results: The rate of incomplete follow-up was very low, with only 3 out of 111 patients (2.7%) in the DCB-combined strategy group and 1 out of 112 patients (0.9%) in the BMS group. At 8 years there were a lower rate of TVR [3.7% vs. 14.3%; hazard ratio (HR): 0.243; 95% confidence interval (CI): 0.081-0.727; P=0.006], and a trend towards lower TLR (2.8% vs. 8.9%; HR: 0.300; 95% CI: 0.083-1.090; P=0.052) in the DCB-combined strategy group. No statistical difference between the DCB-combined strategy and BMS groups were found for all causes of death, deaths from cardiovascular disease, reinfarctions or stent thrombosis. Notably in the DCB-combined strategy group, no episode of stent thrombosis occurred after the first year. Similarly, there were no cardiovascular deaths, TVR and TLR in the DCB-combined strategy group after 5 years. In contrast, during the period from year 5 to 8, the BMS group experienced an additional cardiovascular death, as well as one case of TVR, one case of TLR, and one case of stent thrombosis.
Conclusions: In STEMI patients, the DCB-combined strategy maintains its safety and clinical efficacy over time. Our rates of TVR, TLR, and very late stent thrombosis (VLST) at very long-term are the lowest ever found in a STEMI trial. Further studies are warranted to assess the potential superiority of this novel strategy as compared with new-generation DES to prevent very late events in these patients.
期刊介绍:
The journal ''Cardiovascular Diagnosis and Therapy'' (Print ISSN: 2223-3652; Online ISSN: 2223-3660) accepts basic and clinical science submissions related to Cardiovascular Medicine and Surgery. The mission of the journal is the rapid exchange of scientific information between clinicians and scientists worldwide. To reach this goal, the journal will focus on novel media, using a web-based, digital format in addition to traditional print-version. This includes on-line submission, review, publication, and distribution. The digital format will also allow submission of extensive supporting visual material, both images and video. The website www.thecdt.org will serve as the central hub and also allow posting of comments and on-line discussion. The web-site of the journal will be linked to a number of international web-sites (e.g. www.dxy.cn), which will significantly expand the distribution of its contents.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
