M Virtanen, S Törmälehto, T Partonen, M Elovainio, R Ruuhela, C Hakulinen, K Komulainen, J Airaksinen, A Väänänen, A Koskinen, R Sund
{"title":"Seasonal patterns of sickness absence due to diagnosed mental disorders: a nationwide 12-year register linkage study.","authors":"M Virtanen, S Törmälehto, T Partonen, M Elovainio, R Ruuhela, C Hakulinen, K Komulainen, J Airaksinen, A Väänänen, A Koskinen, R Sund","doi":"10.1017/S2045796023000768","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Although seasonality has been documented for mental disorders, it is unknown whether similar patterns can be observed in employee sickness absence from work due to a wide range of mental disorders with different severity level, and to what extent the rate of change in light exposure plays a role. To address these limitations, we used daily based sickness absence records to examine seasonal patterns in employee sickness absence due to mental disorders.</p><p><strong>Methods: </strong>We used nationwide diagnosis-specific psychiatric sickness absence claims data from 2006 to 2017 for adult individuals aged 16-67 (<i>n</i> = 636,543 sickness absence episodes) in Finland, a high-latitude country with a profound variation in daylength. The smoothed time-series of the ratio of observed and expected (O/E) daily counts of episodes were estimated, adjusted for variation in all-cause sickness absence rates during the year.</p><p><strong>Results: </strong>Unipolar depressive disorders peaked in October-November and dipped in July, with similar associations in all forms of depression. Also, anxiety and non-organic sleep disorders peaked in October-November. Anxiety disorders dipped in January-February and in July-August, while non-organic sleep disorders dipped in April-August. Manic episodes reached a peak from March to July and dipped in September-November and in January-February. Seasonality was not dependent on the severity of the depressive disorder.</p><p><strong>Conclusions: </strong>These results suggest a seasonal variation in sickness absence due to common mental disorders and bipolar disorder, with high peaks in depressive, anxiety and sleep disorders towards the end of the year and a peak in manic episodes starting in spring. Rapid changes in light exposure may contribute to sickness absence due to bipolar disorder. The findings can help clinicians and workplaces prepare for seasonal variations in healthcare needs.</p>","PeriodicalId":11787,"journal":{"name":"Epidemiology and Psychiatric Sciences","volume":"32 ","pages":"e64"},"PeriodicalIF":6.1000,"publicationDate":"2023-11-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7615330/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Epidemiology and Psychiatric Sciences","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1017/S2045796023000768","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PSYCHIATRY","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Although seasonality has been documented for mental disorders, it is unknown whether similar patterns can be observed in employee sickness absence from work due to a wide range of mental disorders with different severity level, and to what extent the rate of change in light exposure plays a role. To address these limitations, we used daily based sickness absence records to examine seasonal patterns in employee sickness absence due to mental disorders.
Methods: We used nationwide diagnosis-specific psychiatric sickness absence claims data from 2006 to 2017 for adult individuals aged 16-67 (n = 636,543 sickness absence episodes) in Finland, a high-latitude country with a profound variation in daylength. The smoothed time-series of the ratio of observed and expected (O/E) daily counts of episodes were estimated, adjusted for variation in all-cause sickness absence rates during the year.
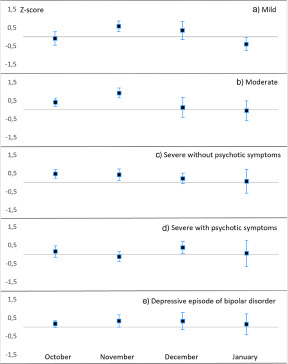
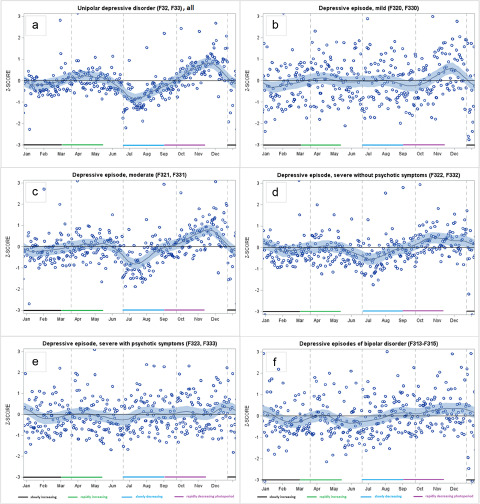
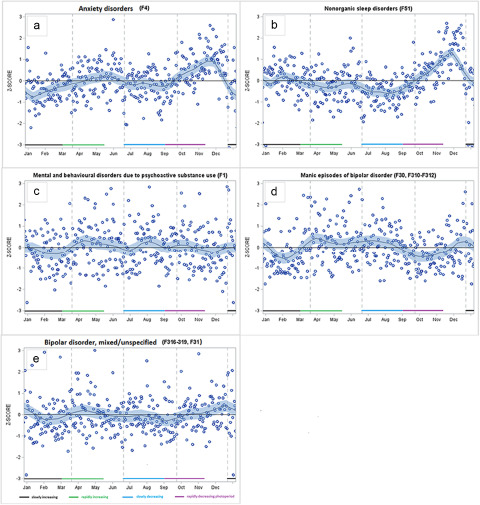
Results: Unipolar depressive disorders peaked in October-November and dipped in July, with similar associations in all forms of depression. Also, anxiety and non-organic sleep disorders peaked in October-November. Anxiety disorders dipped in January-February and in July-August, while non-organic sleep disorders dipped in April-August. Manic episodes reached a peak from March to July and dipped in September-November and in January-February. Seasonality was not dependent on the severity of the depressive disorder.
Conclusions: These results suggest a seasonal variation in sickness absence due to common mental disorders and bipolar disorder, with high peaks in depressive, anxiety and sleep disorders towards the end of the year and a peak in manic episodes starting in spring. Rapid changes in light exposure may contribute to sickness absence due to bipolar disorder. The findings can help clinicians and workplaces prepare for seasonal variations in healthcare needs.
期刊介绍:
Epidemiology and Psychiatric Sciences is a prestigious international, peer-reviewed journal that has been publishing in Open Access format since 2020. Formerly known as Epidemiologia e Psichiatria Sociale and established in 1992 by Michele Tansella, the journal prioritizes highly relevant and innovative research articles and systematic reviews in the areas of public mental health and policy, mental health services and system research, as well as epidemiological and social psychiatry. Join us in advancing knowledge and understanding in these critical fields.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
