Impact of left ventricular end-diastolic pressure as a marker for diastolic dysfunction on long-term outcomes in patients undergoing transcatheter aortic valve replacement
Mariia Emelianova , Vanessa Sciacca , Regine Brinkmann , Smita Scholtz , Volker Rudolph , Sabine Bleiziffer , Tanja K. Rudolph , Muhammed Gerçek , Maria Vanezi
{"title":"Impact of left ventricular end-diastolic pressure as a marker for diastolic dysfunction on long-term outcomes in patients undergoing transcatheter aortic valve replacement","authors":"Mariia Emelianova , Vanessa Sciacca , Regine Brinkmann , Smita Scholtz , Volker Rudolph , Sabine Bleiziffer , Tanja K. Rudolph , Muhammed Gerçek , Maria Vanezi","doi":"10.1016/j.hjc.2023.10.005","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><div>The aim of this study was to investigate the proportion of elevated left ventricular end-diastolic pressure (LVEDP) as an indicator of diastolic function after transcatheter aortic valve replacement (TAVR) and its implication in predicting long-term mortality.</div></div><div><h3>Methods</h3><div>We analyzed retrospectively collected data on 3328 patients with severe aortic stenosis undergoing TAVR in our institution between July 2009 and June 2021. Patients were stratified into two groups based on invasive post-procedural LVEDP measurements: normal (<15 mmHg) vs. elevated (≥15 mmHg) LVEDP.</div></div><div><h3>Results</h3><div>Mean age of the patients was 81.6 years, and 53.3% were female. Elevated post-procedural LVEDP was identified in 2408 (72.3%) patients. The 5-year mortality rates were higher in the group with elevated LVEDP compared with the group with normal LVEDP (27.4% vs. 8.3%, p = 0.01; hazard ratio [HR] 1.22, 95% CI 1.05-1.41). A multivariate model revealed the following independent predictors of mortality after TAVR: post-procedural elevated LVEDP (HR 1.24, 95% CI 1.01-1.53), pre-procedural significant tricuspid regurgitation (HR 1.24, 95% CI 1.02-1.52) and pulmonary hypertension (PH) (HR 1.53, 95% CI 1.26-1.86). In the present study, a significant paravalvular leak after TAVR was not associated with higher mortality (HR 1.45, 95% CI-0.95-2.19, p = 0.75).</div></div><div><h3>Conclusion</h3><div>Elevated post-procedural LVEDP in patients who undergo TAVR is an independent predictor of all-cause mortality. Furthermore, PH and tricuspid regurgitation were also identified as predictors of mortality. These data confirm that diastolic dysfunction is an important predictor of mortality in TAVR and should be considered to guide procedure timing, favoring an early interventional approach and management in aortic stenosis patients.</div></div>","PeriodicalId":55062,"journal":{"name":"Hellenic Journal of Cardiology","volume":"80 ","pages":"Pages 4-11"},"PeriodicalIF":3.0000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hellenic Journal of Cardiology","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1109966623001963","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
The aim of this study was to investigate the proportion of elevated left ventricular end-diastolic pressure (LVEDP) as an indicator of diastolic function after transcatheter aortic valve replacement (TAVR) and its implication in predicting long-term mortality.
Methods
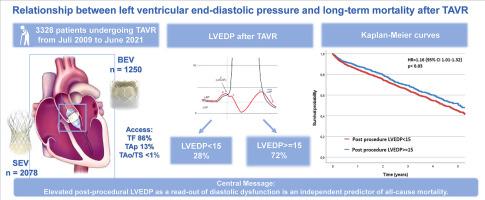
We analyzed retrospectively collected data on 3328 patients with severe aortic stenosis undergoing TAVR in our institution between July 2009 and June 2021. Patients were stratified into two groups based on invasive post-procedural LVEDP measurements: normal (<15 mmHg) vs. elevated (≥15 mmHg) LVEDP.
Results
Mean age of the patients was 81.6 years, and 53.3% were female. Elevated post-procedural LVEDP was identified in 2408 (72.3%) patients. The 5-year mortality rates were higher in the group with elevated LVEDP compared with the group with normal LVEDP (27.4% vs. 8.3%, p = 0.01; hazard ratio [HR] 1.22, 95% CI 1.05-1.41). A multivariate model revealed the following independent predictors of mortality after TAVR: post-procedural elevated LVEDP (HR 1.24, 95% CI 1.01-1.53), pre-procedural significant tricuspid regurgitation (HR 1.24, 95% CI 1.02-1.52) and pulmonary hypertension (PH) (HR 1.53, 95% CI 1.26-1.86). In the present study, a significant paravalvular leak after TAVR was not associated with higher mortality (HR 1.45, 95% CI-0.95-2.19, p = 0.75).
Conclusion
Elevated post-procedural LVEDP in patients who undergo TAVR is an independent predictor of all-cause mortality. Furthermore, PH and tricuspid regurgitation were also identified as predictors of mortality. These data confirm that diastolic dysfunction is an important predictor of mortality in TAVR and should be considered to guide procedure timing, favoring an early interventional approach and management in aortic stenosis patients.
期刊介绍:
The Hellenic Journal of Cardiology (International Edition, ISSN 1109-9666) is the official journal of the Hellenic Society of Cardiology and aims to publish high-quality articles on all aspects of cardiovascular medicine. A primary goal is to publish in each issue a number of original articles related to clinical and basic research. Many of these will be accompanied by invited editorial comments.
Hot topics, such as molecular cardiology, and innovative cardiac imaging and electrophysiological mapping techniques, will appear frequently in the journal in the form of invited expert articles or special reports. The Editorial Committee also attaches great importance to subjects related to continuing medical education, the implementation of guidelines and cost effectiveness in cardiology.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
