{"title":"End-expiratory Occlusion Test and Mini-fluid Challenge Test for Predicting Fluid Responsiveness in Acute Circulatory Failure.","authors":"Velmurugan Selvam, Dilip Shende, Rahul Kumar Anand, Lokesh Kashyap, Bikash Ranjan Ray","doi":"10.4103/jets.jets_44_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Predicting which patients with acute circulatory failure will respond to the fluid by an increase in cardiac output is a daily challenge. End-expiratory occlusion test (EEOT) and mini-fluid challenge (MFC) can be used for assessing fluid responsiveness in patients with spontaneous breathing activity, cardiac arrhythmias, low-tidal volume and/or low lung compliance.</p><p><strong>Methods: </strong>The objective of the study is to evaluate the value of EEOT and MFC-induced rise in left ventricular outflow tract (LVOT) velocity time integral (VTI) in predicting fluid responsiveness in acute circulatory failure in comparison to the passive leg-raising (PLR) test. Hundred critically ill ventilated and sedated patients with acute circulatory failure were studied. LVOT VTI was measured by transthoracic echocardiography before and after EEOT (interrupting the ventilator at end-expiration over 15 s), and before and after MFC (100 ml of Ringer lactate was infused over 1 min). The variation of LVOT VTI after EEOT and the MFC was calculated from the baseline. Sensitivity, specificity, and area under the receiver-operating characteristic (AUROC) curve of LVOT VTI after EEOT and MFC to predict fluid responsiveness were determined.</p><p><strong>Results: </strong>After PLR, stroke volume (SV) increased by ≥12% in 49 patients, who were defined as responders and 34 patients in whom the increase in SV <12% were defined as nonresponders. A cutoff of 9.1% Change in VTI after MFC (ΔVTI<sub>MFC</sub>) predicted fluid responsiveness with an AUROC of 0.96 (<i>P</i> < 0.001) with sensitivity and specificity of 91.5% and 88.9%, respectively. Change in VTI after EEOT (ΔVTI<sub>EEOT</sub>) >4.3% predicted fluid responsiveness with sensitivity and specificity 89.4% and 88.9%, respectively, with an AUROC of 0.97 (<i>P</i> < 0.001), but in 17 patients, EEOT was not possible because triggering of the ventilator by the patient's inspiratory effort.</p><p><strong>Conclusion: </strong>In conclusion, in mechanically ventilated patients with acute circulatory failure Δ VTI<sub>MFC</sub> and Δ VTI <sub>EEOT</sub> accurately predicts fluid responsiveness.</p>","PeriodicalId":18752,"journal":{"name":"Modern Physics Letters A","volume":"32 1","pages":"109-115"},"PeriodicalIF":1.6000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10661572/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Modern Physics Letters A","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jets.jets_44_23","RegionNum":4,"RegionCategory":"物理与天体物理","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/10 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ASTRONOMY & ASTROPHYSICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Predicting which patients with acute circulatory failure will respond to the fluid by an increase in cardiac output is a daily challenge. End-expiratory occlusion test (EEOT) and mini-fluid challenge (MFC) can be used for assessing fluid responsiveness in patients with spontaneous breathing activity, cardiac arrhythmias, low-tidal volume and/or low lung compliance.
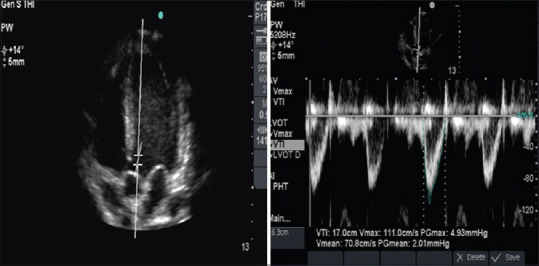
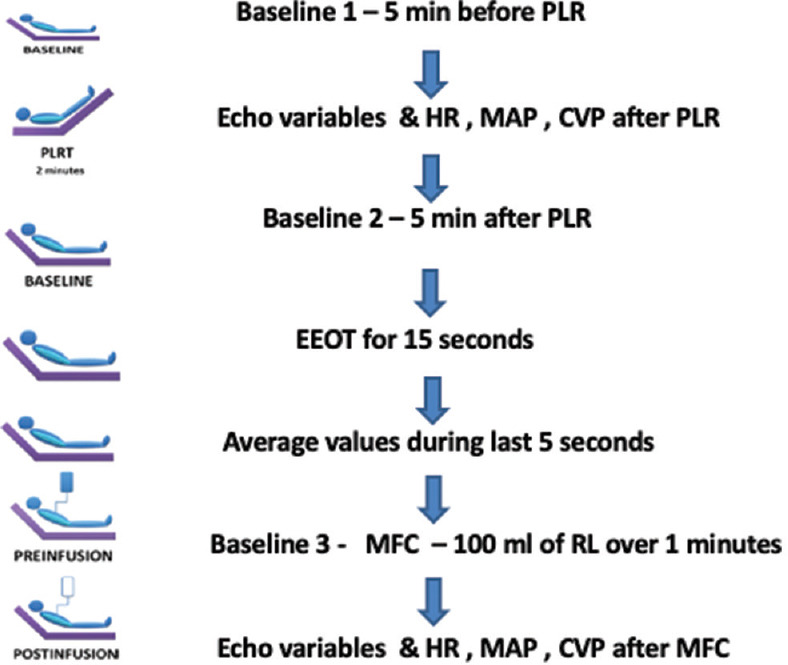
Methods: The objective of the study is to evaluate the value of EEOT and MFC-induced rise in left ventricular outflow tract (LVOT) velocity time integral (VTI) in predicting fluid responsiveness in acute circulatory failure in comparison to the passive leg-raising (PLR) test. Hundred critically ill ventilated and sedated patients with acute circulatory failure were studied. LVOT VTI was measured by transthoracic echocardiography before and after EEOT (interrupting the ventilator at end-expiration over 15 s), and before and after MFC (100 ml of Ringer lactate was infused over 1 min). The variation of LVOT VTI after EEOT and the MFC was calculated from the baseline. Sensitivity, specificity, and area under the receiver-operating characteristic (AUROC) curve of LVOT VTI after EEOT and MFC to predict fluid responsiveness were determined.
Results: After PLR, stroke volume (SV) increased by ≥12% in 49 patients, who were defined as responders and 34 patients in whom the increase in SV <12% were defined as nonresponders. A cutoff of 9.1% Change in VTI after MFC (ΔVTIMFC) predicted fluid responsiveness with an AUROC of 0.96 (P < 0.001) with sensitivity and specificity of 91.5% and 88.9%, respectively. Change in VTI after EEOT (ΔVTIEEOT) >4.3% predicted fluid responsiveness with sensitivity and specificity 89.4% and 88.9%, respectively, with an AUROC of 0.97 (P < 0.001), but in 17 patients, EEOT was not possible because triggering of the ventilator by the patient's inspiratory effort.
Conclusion: In conclusion, in mechanically ventilated patients with acute circulatory failure Δ VTIMFC and Δ VTI EEOT accurately predicts fluid responsiveness.
期刊介绍:
This letters journal, launched in 1986, consists of research papers covering current research developments in Gravitation, Cosmology, Astrophysics, Nuclear Physics, Particles and Fields, Accelerator physics, and Quantum Information. A Brief Review section has also been initiated with the purpose of publishing short reports on the latest experimental findings and urgent new theoretical developments.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
