Song Ge, Yuting Song, Jiale Hu, Xianping Tang, Junxin Li, Linda Dune
{"title":"The development and impact of adopting electronic health records in the United States: A brief overview and implications for nursing education","authors":"Song Ge, Yuting Song, Jiale Hu, Xianping Tang, Junxin Li, Linda Dune","doi":"10.1002/hcs2.21","DOIUrl":null,"url":null,"abstract":"<p>At present, health-care systems in the United States face enormous challenges in providing quality care, characterized by safe, effective, efficient, patient-centered, timely, and equitable care while containing health-care costs [<span>1</span>, <span>2</span>]. To understand and address patients' increasingly complicated health-care needs, we need safe access to quality information that is characterized by integrity, reliability, and accuracy [<span>3</span>], and establish mutually beneficial relationships among a multidisciplinary team of professionals [<span>4</span>]. Traditional paper-based clinical workflow produces many issues such as illegible handwriting, inconvenient access, the possibility of computational prescribing errors, inadequate patient hand-offs, and drug administration errors. These problems can lead to medical errors, omissions, and duplications and, ultimately, poor patient outcomes and compromised quality of care [<span>2</span>].</p><p>Electronic health records (EHR) is a major achievement in the health information technology [<span>5</span>]. It is deemed a promising solution to improve the interoperability of patients' information across health-care settings and achieve a more cost-effective, safer, and higher quality of care [<span>3</span>, <span>6</span>]. Electronic medical records (EMR) is a different concept from EHR; thus, the two terms cannot be used interchangeably. The EMR is the official record produced by hospitals and other ambulatory settings that serves as the EHR's data source. EMR is a prerequisite for EHR [<span>7</span>]. EHR refers to systematic documentation of patients' health status and health care in a secured digital format [<span>8</span>]. It indicates that patients' health information can not only be stored but also be transmitted and accessed by authorized interdisciplinary professionals across health-care settings in patients' health-care continuum. In addition, authorized non-health-care professionals, including insurers, the government, and researchers can also have access to patients' health information as well.</p><p>With EHR, patients can have greater autonomy over their care, and clinicians may better understand patients' medical history and coordinate care with other interdisciplinary professionals with fewer barriers [<span>2</span>]. EHR can also provide data for a variety of other purposes such as providing data for research, population-based interventions, and reporting quality-related measures [<span>9</span>]. Thus, this technological innovation benefits not only patients but also healthcare providers, administrative officers, researchers, and professionals from a variety of disciplines [<span>10</span>].</p><p>The adoption of EHR in the United States started early and was accelerated by laws and regulations. In 2004, US President George W. Bush proposed a plan that most Americans would have EHR by 2014. He stated that computerizing health records could help clinicians avoid dangerous medical mistakes, reduce costs, and improve patients' care [<span>11</span>]. Later, President Obama continued this effort by proposing the American Recovery and Reinvestment Act of 2009 [<span>12</span>]. This policy included the Health Information Technology for Economic and Clinical Health (HITECH) Act to use Medicare and Medicaid to provide explicit reimbursement and penalties incentives for health organizations and providers to adopt EHR meaningfully within a specific time frame [<span>10</span>, <span>13</span>]. Initiating this act, the federal government committed unprecedented resources to support the adoption of EHR [<span>10</span>]. The HITECH Act could be considered “the most significant driver” to encourage the adoption of EHR in the United States before the COVID-19 pandemic [<span>14</span>]. It was important to note that not all EHR were eligible for reimbursement. The HITECH act specifies that health-care providers and organizations must implement all the EHR's core objectives before selecting five of ten additional ones to accomplish during the first 2 years to be eligible for reimbursement. The fundamental tasks that supported better health care were included in the key objectives defined by the HITECH act and included the data entry and many software-based clinical decision support systems (DSS) [<span>10</span>]. The optional objectives gave providers the opportunity to make choices based on their circumstances. A wide spectrum of health-care companies in the United States has implemented EHR after more than 10 years, despite the fact that the technology and standards are constantly changing and there are still acceptance barriers. [<span>15</span>]. In 2001, only 18% of physicians used EHR, compared with over 80% in 2016 [<span>16</span>]. Moreover, according to the Healthcare Information and Management Systems Society (HIMSS) Analytics 2015 Report, 1313 US hospitals have achieved fully implementation of physician documentation, robust clinical DSS, and electronic access to medical imaging (Stage 6) [<span>17</span>] (Figure 1).</p><p>The coronavirus disease 2019 (COVID-19) pandemic that has occurred since 2020 has had an unprecedented impact on the adoption of EHR in the United States. As EHR offered convenience, safety, quicker results reporting, and virtual visits, EHR was highly demanded during COVID-19 when people's life was disrupted. In addition, with the order of President Trump, under the Stafford Act and the National Emergencies Act, the Center for Medicare and Medicaid temporarily expanded coverage for telehealth and virtual care visits [<span>18</span>]. Certain regulatory changes also took place, such as allowing providers to practice across state lines. All these pandemic-related changes led to leaps in the adoption of EHR. The change was unprecedented. For example, following March 13, 2020, Intermountain Health saw a rise in telehealth visits from about 100 per month to over 50,000 per week [<span>19</span>]. Overall, COVID-19 caused extensive short-term and long-term changes in people's attitudes toward as well as demand for HER.</p><p>The detailed components of EHR are shown in Table 1.</p><p>Using EHR to improve healthcare has been a strategy that raises many countries' attention and efforts because of EHR's vast potential and functionalities. However, this is never an easy process and can be viewed as a revolution due to its complexities and scope of change. In this review, we identified several barriers to its adoption from financial, technical, and human aspects. Healthcare institutions should carefully attend to these considerations if they plan to adopt EHR. Rushing this process does not help implement such a large-scale campaign and could lead to worse rather than better outcomes, as illustrated by many earlier studies mentioned above. In particular, hospitals in many developing countries are at an early stage of EHR adoption [<span>39</span>] with a tremendous amount of work that needs to be done. Legislation should be in place regarding guidelines and standards for EHR that are allowed to be implemented with particular attention to interoperability among distinctive. Making EHR systems become interoperability is a widespread challenge. Legislation could facilitate the adoption of EHR by providing health-care agencies with incentives and facilitators to implement specific instructions.</p><p>Meanwhile, health-care agencies should develop an appropriate timeline to adopt EHR, including (a) Identifying the information needs of their organization, (b) understanding the current market of EHR market, and (c) assigning interdisciplinary expertise to choose the desired system among a vast potential selection of vendors and systems, (d) carefully examining features of EHR, (e) getting the hardware ready, (f) adjusting the EHR to fit the need of their specific organization, (g) carefully train personnel, (h) decreasing users' resistance by providing robust and ongoing support, and (i) maintaining and updating the system at regular basis. It is also essential to develop mechanisms to evaluate the impact of EHR on healthcare professionals' workflow efficiency, quality of care, and patient outcomes so that any mistake and weakness can be caught early. Input from multidisciplinary teams is valuable and needed because each profession will bring unique perspectives and have special needs for EMR functions. Overall, we not only need adoption but more integration of EHR within the daily workflow of healthcare agencies and production of better patient outcomes.</p><p>The wide disparity in nurses' informatics competence has negatively affected their utilization of EHR [<span>40</span>]. Nurses need to be willing to learn the strengths and features of EHR over the traditional paper approach and constantly improve their informatics competence to adapt to the changing technology such as big data, artificial intelligence, robotics, and telehealth. This is particularly important during the COVID-19 pandemic when remote diagnosis is expanding quickly. Nurses' EHR learning process can start early to achieve the best results. Nursing students should develop informatics competence in their education. Nursing educators should be aware that fostering a favorable attitude toward using EHR and elevating the perceived value in their nursing students is crucial for improving their acceptance of using them [<span>41</span>]. However, nursing educators from academic institutions are frequently left out of the deployment of EHR themselves and nursing schools often lack EHR education resources [<span>42</span>]. Moreover, a consensus is lacking on the content of information education for bachelor of science in nursing (BSN) students [<span>43</span>]. Thus, the integration of informatics into BSN education has been relatively slow [<span>40</span>]. Many new graduate nurses were not healthcare informatics competent [<span>42</span>].</p><p>Nursing educators must develop effective strategies to incorporate informatics into nursing education and make the education content pragmatic, relevant, and appealing to nursing students. Important concepts should be included in the curriculum, such as the development of EHR, its impact on the health-care system, examples of technology and information systems that are effective and safe within various practice settings, and how to safeguard patients' information. In addition, researchers also found that a simulated EHR curriculum is an effective and engaging approach to teaching students EHR skills and organizing charts leading to a safe, effective, and high-quality patient care [<span>44</span>]. In a simulated EHR curriculum, students draft orders and prescriptions using an EHR training platform, develop an evidence-based nursing care plan, and conduct a small-group review of their work after viewing a virtual medical record of a complex patient with chronic conditions and compromised care.</p><p>Nurses should be competent to use EHR at workplaces after a rigorous selection of the appropriate EHR system in their health-care agency and relevant support provided. As the frontier of healthcare, nurses have great opportunities to participate in this significant revolution. Nurses could work during the preinstallation phase such as helping the agency choose the most suitable system, adjusting the system to the need of their agency with their expertise, encouraging and training their colleagues for adoption, and assisting their agency in evaluating the quality, adoption, and impact of the system. Ultimately, with everyone's efforts, the system will provide all health-care professionals, including nurses better working processes and care outcomes for patients if integrated well with the agency.</p><p><b>Song Ge</b>: Conceptualization (equal); Investigation (equal); Methodology (equal). <b>Yuting Song</b>: Conceptualization (equal); Resources (equal). <b>Jiale Hu</b>: Resources (equal); Software (equal); Supervision (equal). <b>Xianping Tang</b>: Investigation (equal); Software (equal); Supervision (equal). <b>Junxin Li</b>: Conceptualization (equal); Data curation (equal); Formal analysis (equal); Writing – original draft (equal); Writing – review & editing (equal). <b>Linda Dune</b>: Formal analysis (equal); Funding acquisition (equal).</p><p>The authors declare no conflict of interest.</p><p>Not Applicable.</p><p>Not Applicable.</p>","PeriodicalId":100601,"journal":{"name":"Health Care Science","volume":"1 3","pages":"186-192"},"PeriodicalIF":3.3000,"publicationDate":"2022-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hcs2.21","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Care Science","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hcs2.21","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
At present, health-care systems in the United States face enormous challenges in providing quality care, characterized by safe, effective, efficient, patient-centered, timely, and equitable care while containing health-care costs [1, 2]. To understand and address patients' increasingly complicated health-care needs, we need safe access to quality information that is characterized by integrity, reliability, and accuracy [3], and establish mutually beneficial relationships among a multidisciplinary team of professionals [4]. Traditional paper-based clinical workflow produces many issues such as illegible handwriting, inconvenient access, the possibility of computational prescribing errors, inadequate patient hand-offs, and drug administration errors. These problems can lead to medical errors, omissions, and duplications and, ultimately, poor patient outcomes and compromised quality of care [2].
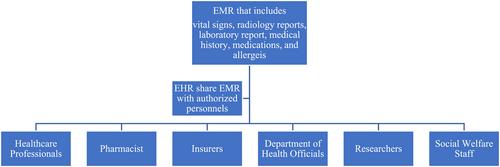
Electronic health records (EHR) is a major achievement in the health information technology [5]. It is deemed a promising solution to improve the interoperability of patients' information across health-care settings and achieve a more cost-effective, safer, and higher quality of care [3, 6]. Electronic medical records (EMR) is a different concept from EHR; thus, the two terms cannot be used interchangeably. The EMR is the official record produced by hospitals and other ambulatory settings that serves as the EHR's data source. EMR is a prerequisite for EHR [7]. EHR refers to systematic documentation of patients' health status and health care in a secured digital format [8]. It indicates that patients' health information can not only be stored but also be transmitted and accessed by authorized interdisciplinary professionals across health-care settings in patients' health-care continuum. In addition, authorized non-health-care professionals, including insurers, the government, and researchers can also have access to patients' health information as well.
With EHR, patients can have greater autonomy over their care, and clinicians may better understand patients' medical history and coordinate care with other interdisciplinary professionals with fewer barriers [2]. EHR can also provide data for a variety of other purposes such as providing data for research, population-based interventions, and reporting quality-related measures [9]. Thus, this technological innovation benefits not only patients but also healthcare providers, administrative officers, researchers, and professionals from a variety of disciplines [10].
The adoption of EHR in the United States started early and was accelerated by laws and regulations. In 2004, US President George W. Bush proposed a plan that most Americans would have EHR by 2014. He stated that computerizing health records could help clinicians avoid dangerous medical mistakes, reduce costs, and improve patients' care [11]. Later, President Obama continued this effort by proposing the American Recovery and Reinvestment Act of 2009 [12]. This policy included the Health Information Technology for Economic and Clinical Health (HITECH) Act to use Medicare and Medicaid to provide explicit reimbursement and penalties incentives for health organizations and providers to adopt EHR meaningfully within a specific time frame [10, 13]. Initiating this act, the federal government committed unprecedented resources to support the adoption of EHR [10]. The HITECH Act could be considered “the most significant driver” to encourage the adoption of EHR in the United States before the COVID-19 pandemic [14]. It was important to note that not all EHR were eligible for reimbursement. The HITECH act specifies that health-care providers and organizations must implement all the EHR's core objectives before selecting five of ten additional ones to accomplish during the first 2 years to be eligible for reimbursement. The fundamental tasks that supported better health care were included in the key objectives defined by the HITECH act and included the data entry and many software-based clinical decision support systems (DSS) [10]. The optional objectives gave providers the opportunity to make choices based on their circumstances. A wide spectrum of health-care companies in the United States has implemented EHR after more than 10 years, despite the fact that the technology and standards are constantly changing and there are still acceptance barriers. [15]. In 2001, only 18% of physicians used EHR, compared with over 80% in 2016 [16]. Moreover, according to the Healthcare Information and Management Systems Society (HIMSS) Analytics 2015 Report, 1313 US hospitals have achieved fully implementation of physician documentation, robust clinical DSS, and electronic access to medical imaging (Stage 6) [17] (Figure 1).
The coronavirus disease 2019 (COVID-19) pandemic that has occurred since 2020 has had an unprecedented impact on the adoption of EHR in the United States. As EHR offered convenience, safety, quicker results reporting, and virtual visits, EHR was highly demanded during COVID-19 when people's life was disrupted. In addition, with the order of President Trump, under the Stafford Act and the National Emergencies Act, the Center for Medicare and Medicaid temporarily expanded coverage for telehealth and virtual care visits [18]. Certain regulatory changes also took place, such as allowing providers to practice across state lines. All these pandemic-related changes led to leaps in the adoption of EHR. The change was unprecedented. For example, following March 13, 2020, Intermountain Health saw a rise in telehealth visits from about 100 per month to over 50,000 per week [19]. Overall, COVID-19 caused extensive short-term and long-term changes in people's attitudes toward as well as demand for HER.
The detailed components of EHR are shown in Table 1.
Using EHR to improve healthcare has been a strategy that raises many countries' attention and efforts because of EHR's vast potential and functionalities. However, this is never an easy process and can be viewed as a revolution due to its complexities and scope of change. In this review, we identified several barriers to its adoption from financial, technical, and human aspects. Healthcare institutions should carefully attend to these considerations if they plan to adopt EHR. Rushing this process does not help implement such a large-scale campaign and could lead to worse rather than better outcomes, as illustrated by many earlier studies mentioned above. In particular, hospitals in many developing countries are at an early stage of EHR adoption [39] with a tremendous amount of work that needs to be done. Legislation should be in place regarding guidelines and standards for EHR that are allowed to be implemented with particular attention to interoperability among distinctive. Making EHR systems become interoperability is a widespread challenge. Legislation could facilitate the adoption of EHR by providing health-care agencies with incentives and facilitators to implement specific instructions.
Meanwhile, health-care agencies should develop an appropriate timeline to adopt EHR, including (a) Identifying the information needs of their organization, (b) understanding the current market of EHR market, and (c) assigning interdisciplinary expertise to choose the desired system among a vast potential selection of vendors and systems, (d) carefully examining features of EHR, (e) getting the hardware ready, (f) adjusting the EHR to fit the need of their specific organization, (g) carefully train personnel, (h) decreasing users' resistance by providing robust and ongoing support, and (i) maintaining and updating the system at regular basis. It is also essential to develop mechanisms to evaluate the impact of EHR on healthcare professionals' workflow efficiency, quality of care, and patient outcomes so that any mistake and weakness can be caught early. Input from multidisciplinary teams is valuable and needed because each profession will bring unique perspectives and have special needs for EMR functions. Overall, we not only need adoption but more integration of EHR within the daily workflow of healthcare agencies and production of better patient outcomes.
The wide disparity in nurses' informatics competence has negatively affected their utilization of EHR [40]. Nurses need to be willing to learn the strengths and features of EHR over the traditional paper approach and constantly improve their informatics competence to adapt to the changing technology such as big data, artificial intelligence, robotics, and telehealth. This is particularly important during the COVID-19 pandemic when remote diagnosis is expanding quickly. Nurses' EHR learning process can start early to achieve the best results. Nursing students should develop informatics competence in their education. Nursing educators should be aware that fostering a favorable attitude toward using EHR and elevating the perceived value in their nursing students is crucial for improving their acceptance of using them [41]. However, nursing educators from academic institutions are frequently left out of the deployment of EHR themselves and nursing schools often lack EHR education resources [42]. Moreover, a consensus is lacking on the content of information education for bachelor of science in nursing (BSN) students [43]. Thus, the integration of informatics into BSN education has been relatively slow [40]. Many new graduate nurses were not healthcare informatics competent [42].
Nursing educators must develop effective strategies to incorporate informatics into nursing education and make the education content pragmatic, relevant, and appealing to nursing students. Important concepts should be included in the curriculum, such as the development of EHR, its impact on the health-care system, examples of technology and information systems that are effective and safe within various practice settings, and how to safeguard patients' information. In addition, researchers also found that a simulated EHR curriculum is an effective and engaging approach to teaching students EHR skills and organizing charts leading to a safe, effective, and high-quality patient care [44]. In a simulated EHR curriculum, students draft orders and prescriptions using an EHR training platform, develop an evidence-based nursing care plan, and conduct a small-group review of their work after viewing a virtual medical record of a complex patient with chronic conditions and compromised care.
Nurses should be competent to use EHR at workplaces after a rigorous selection of the appropriate EHR system in their health-care agency and relevant support provided. As the frontier of healthcare, nurses have great opportunities to participate in this significant revolution. Nurses could work during the preinstallation phase such as helping the agency choose the most suitable system, adjusting the system to the need of their agency with their expertise, encouraging and training their colleagues for adoption, and assisting their agency in evaluating the quality, adoption, and impact of the system. Ultimately, with everyone's efforts, the system will provide all health-care professionals, including nurses better working processes and care outcomes for patients if integrated well with the agency.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
