{"title":"Mounier-Kuhn Syndrome.","authors":"Irfan Ismail Ayub, Krishnamoorthy Vengadakrishnan","doi":"10.4046/trd.2022.0123","DOIUrl":null,"url":null,"abstract":"It is identical to the Creative Commons Attribution NonCommercial License (http:// creativecommons.org/licenses/ by-nc/4.0/). Sixty-two-year-old male presented with increasing cough, purulent sputum, and breathlessness for 3 days. Over the last 30 years, the patient has had a recurring cough with sputum, often interrupted by exacerbations, requiring multiple outpatient and emergency visits, and on several occasions, admissions for antibiotics, oxygen, and bronchodilator therapy. Clinical examination revealed tachypnoea with peripheral saturation of 91%, tachycardia, pallor, digital clubbing, with bilateral crackles, and wheeze on chest auscultation. Blood investigations and arterial blood gas analysis revealed anaemia and hypoxemia, respectively. Sputum microbiology, sweat chloride, and serum immunoglobulin profile were non-contributory. Chest radiograph showed bilateral lower zone cystic changes (yellow circles) with airspace opacities (white arrows) (Figure 1). A computed tomography scan of the chest revealed tracheomegaly (tracheal diameter 31.29 mm) with multiple tracheal and bronchial wall diverticula (red arrows), upper lobe emphysema (E), bilateral bronchiectasis (yellow arrows), and right lung consolidation (P) (Figure 2A, B). Flexible bronchoscopy confirmed multiple tracheal and bronchial wall diverticulosis (white arrows), with visible overlying atrophied longitudinal smooth muscle (black arrows), consistent with Mounier-Kuhn syndrome (Figure 2C). The bronchoalveolar lavage from the middle lobe grew Klebsiella pneumoniae. He was discharged after clinical and radiological results showed improvement following appropriate antibiotic, oxygen, and bronchodilator therapy. He continues having reasonable symptom control with regular home nebulized bronchodilator therapy and chest physiotherapy, and","PeriodicalId":23368,"journal":{"name":"Tuberculosis and Respiratory Diseases","volume":"86 1","pages":"59-60"},"PeriodicalIF":3.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0e/c9/trd-2022-0123.PMC9816488.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tuberculosis and Respiratory Diseases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4046/trd.2022.0123","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 1
Abstract
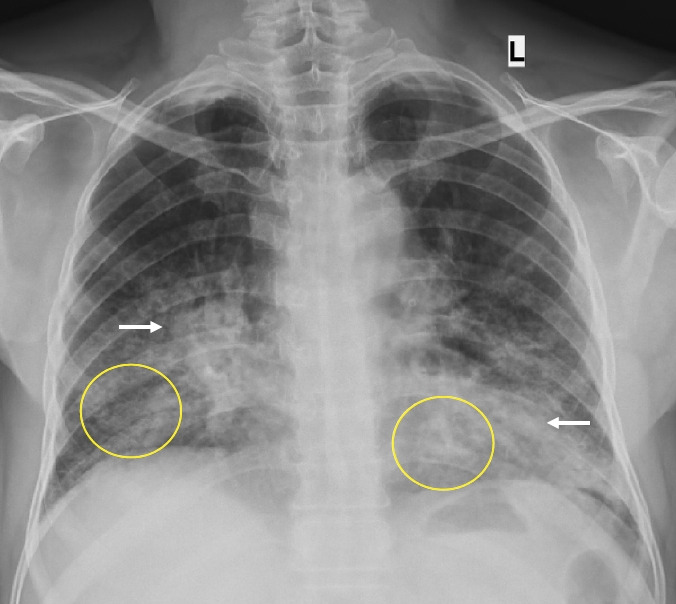
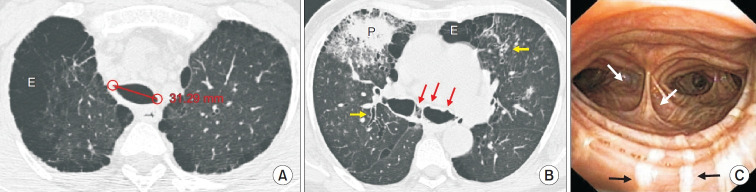
It is identical to the Creative Commons Attribution NonCommercial License (http:// creativecommons.org/licenses/ by-nc/4.0/). Sixty-two-year-old male presented with increasing cough, purulent sputum, and breathlessness for 3 days. Over the last 30 years, the patient has had a recurring cough with sputum, often interrupted by exacerbations, requiring multiple outpatient and emergency visits, and on several occasions, admissions for antibiotics, oxygen, and bronchodilator therapy. Clinical examination revealed tachypnoea with peripheral saturation of 91%, tachycardia, pallor, digital clubbing, with bilateral crackles, and wheeze on chest auscultation. Blood investigations and arterial blood gas analysis revealed anaemia and hypoxemia, respectively. Sputum microbiology, sweat chloride, and serum immunoglobulin profile were non-contributory. Chest radiograph showed bilateral lower zone cystic changes (yellow circles) with airspace opacities (white arrows) (Figure 1). A computed tomography scan of the chest revealed tracheomegaly (tracheal diameter 31.29 mm) with multiple tracheal and bronchial wall diverticula (red arrows), upper lobe emphysema (E), bilateral bronchiectasis (yellow arrows), and right lung consolidation (P) (Figure 2A, B). Flexible bronchoscopy confirmed multiple tracheal and bronchial wall diverticulosis (white arrows), with visible overlying atrophied longitudinal smooth muscle (black arrows), consistent with Mounier-Kuhn syndrome (Figure 2C). The bronchoalveolar lavage from the middle lobe grew Klebsiella pneumoniae. He was discharged after clinical and radiological results showed improvement following appropriate antibiotic, oxygen, and bronchodilator therapy. He continues having reasonable symptom control with regular home nebulized bronchodilator therapy and chest physiotherapy, and



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
