Rebecca C Gosling, Gareth Williams, Abdulaziz Al Baraikan, Samer Alabed, Eylem Levelt, Amrit Chowdhary, Peter P Swoboda, Ian Halliday, D Rodney Hose, Julian P Gunn, John P Greenwood, Sven Plein, Andrew J Swift, James M Wild, Pankaj Garg, Paul D Morris
{"title":"Quantifying Myocardial Blood Flow and Resistance Using 4D-Flow Cardiac Magnetic Resonance Imaging.","authors":"Rebecca C Gosling, Gareth Williams, Abdulaziz Al Baraikan, Samer Alabed, Eylem Levelt, Amrit Chowdhary, Peter P Swoboda, Ian Halliday, D Rodney Hose, Julian P Gunn, John P Greenwood, Sven Plein, Andrew J Swift, James M Wild, Pankaj Garg, Paul D Morris","doi":"10.1155/2023/3875924","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Ischaemia with nonobstructive coronary arteries is most commonly caused by coronary microvascular dysfunction but remains difficult to diagnose without invasive testing. Myocardial blood flow (MBF) can be quantified noninvasively on stress perfusion cardiac magnetic resonance (CMR) or positron emission tomography but neither is routinely used in clinical practice due to practical and technical constraints. Quantification of coronary sinus (CS) flow may represent a simpler method for CMR MBF quantification. 4D flow CMR offers comprehensive intracardiac and transvalvular flow quantification. However, it is feasibility to quantify MBF remains unknown.</p><p><strong>Methods: </strong>Patients with acute myocardial infarction (MI) and healthy volunteers underwent CMR. The CS contours were traced from the 2-chamber view. A reformatted phase contrast plane was generated through the CS, and flow was quantified using 4D flow CMR over the cardiac cycle and normalised for myocardial mass. MBF and resistance (MyoR) was determined in ten healthy volunteers, ten patients with myocardial infarction (MI) without microvascular obstruction (MVO), and ten with known MVO.</p><p><strong>Results: </strong>MBF was quantified in all 30 subjects. MBF was highest in healthy controls (123.8 ± 48.4 mL/min), significantly lower in those with MI (85.7 ± 30.5 mL/min), and even lower in those with MI and MVO (67.9 ± 29.2 mL/min/) (<i>P</i> < 0.01 for both differences). Compared with healthy controls, MyoR was higher in those with MI and even higher in those with MI and MVO (0.79 (±0.35) versus 1.10 (±0.50) versus 1.50 (±0.69), <i>P</i>=0.02).</p><p><strong>Conclusions: </strong>MBF and MyoR can be quantified from 4D flow CMR. Resting MBF was reduced in patients with MI and MVO.</p>","PeriodicalId":9494,"journal":{"name":"Cardiology Research and Practice","volume":"2023 ","pages":"3875924"},"PeriodicalIF":1.8000,"publicationDate":"2023-02-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9911256/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology Research and Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2023/3875924","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Ischaemia with nonobstructive coronary arteries is most commonly caused by coronary microvascular dysfunction but remains difficult to diagnose without invasive testing. Myocardial blood flow (MBF) can be quantified noninvasively on stress perfusion cardiac magnetic resonance (CMR) or positron emission tomography but neither is routinely used in clinical practice due to practical and technical constraints. Quantification of coronary sinus (CS) flow may represent a simpler method for CMR MBF quantification. 4D flow CMR offers comprehensive intracardiac and transvalvular flow quantification. However, it is feasibility to quantify MBF remains unknown.
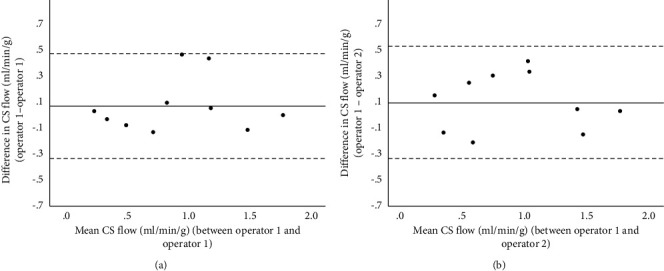
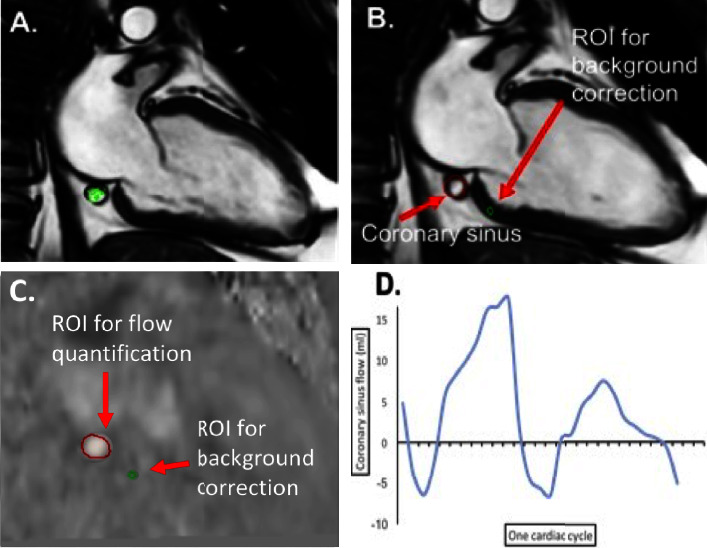
Methods: Patients with acute myocardial infarction (MI) and healthy volunteers underwent CMR. The CS contours were traced from the 2-chamber view. A reformatted phase contrast plane was generated through the CS, and flow was quantified using 4D flow CMR over the cardiac cycle and normalised for myocardial mass. MBF and resistance (MyoR) was determined in ten healthy volunteers, ten patients with myocardial infarction (MI) without microvascular obstruction (MVO), and ten with known MVO.
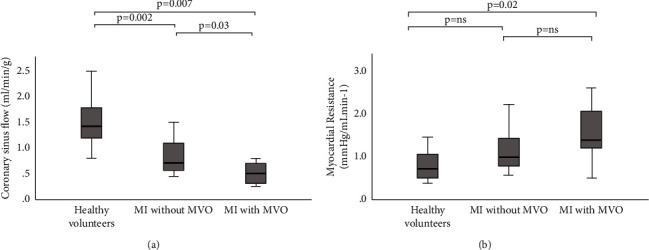
Results: MBF was quantified in all 30 subjects. MBF was highest in healthy controls (123.8 ± 48.4 mL/min), significantly lower in those with MI (85.7 ± 30.5 mL/min), and even lower in those with MI and MVO (67.9 ± 29.2 mL/min/) (P < 0.01 for both differences). Compared with healthy controls, MyoR was higher in those with MI and even higher in those with MI and MVO (0.79 (±0.35) versus 1.10 (±0.50) versus 1.50 (±0.69), P=0.02).
Conclusions: MBF and MyoR can be quantified from 4D flow CMR. Resting MBF was reduced in patients with MI and MVO.
期刊介绍:
Cardiology Research and Practice is a peer-reviewed, Open Access journal that publishes original research articles, review articles, and clinical studies that focus on the diagnosis and treatment of cardiovascular disease. The journal welcomes submissions related to systemic hypertension, arrhythmia, congestive heart failure, valvular heart disease, vascular disease, congenital heart disease, and cardiomyopathy.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
