Post hoc analysis examining symptom severity reduction and symptom absence during food challenges in individuals who underwent oral immunotherapy for peanut allergy: results from three trials.
Katharina Blumchen, Andreas Kleinheinz, Ludger Klimek, Kirsten Beyer, Aikaterini Anagnostou, Christian Vogelberg, Sergejus Butovas, Robert Ryan, David Norval, Stefan Zeitler, George Du Toit
{"title":"Post hoc analysis examining symptom severity reduction and symptom absence during food challenges in individuals who underwent oral immunotherapy for peanut allergy: results from three trials.","authors":"Katharina Blumchen, Andreas Kleinheinz, Ludger Klimek, Kirsten Beyer, Aikaterini Anagnostou, Christian Vogelberg, Sergejus Butovas, Robert Ryan, David Norval, Stefan Zeitler, George Du Toit","doi":"10.1186/s13223-023-00757-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Peanut allergy and its current management, involving peanut avoidance and use of rescue medication during instances of accidental exposure, are burdensome to patients and their caregivers and can be a source of stress, uncertainty, and restriction. Physicians may also be frustrated with a lack of effective and safe treatments other than avoidance in the current management of peanut allergy. Efficacy, determined using double-blind, placebo-controlled food challenges (DBPCFCs), of oral immunotherapy with peanut (Arachis hypogaea) allergen powder-dnfp (PTAH; Palforzia<sup>®</sup>) was demonstrated versus placebo in children and adolescents aged 4 to 17 years in multiple phase 3 trials; continued benefit of PTAH was shown in a follow-on trial. The DBPCFC is a reproducible, rigorous, and clinically meaningful assessment accepted by regulatory authorities to evaluate the level of tolerance as an endpoint for accidental exposures to peanut in real life. It also provides useful clinical and patient-relevant information, including the amount of peanut protein an individual with peanut allergy can consume without experiencing dose-limiting symptoms, severity of symptoms, and organs affected upon ingestion of peanut protein. We explored symptoms of peanut exposure during DBPCFCs from phase 3 and follow-on trials of PTAH to further characterize treatment efficacy from a perspective relevant to patients, caregivers, and clinicians.</p><p><strong>Methods: </strong>Symptom data recorded during screening and/or exit DBPCFCs from participants aged 4 to 17 years receiving PTAH or placebo were examined post hoc across three PTAH trials (PALISADE [ARC003], ARC004 [PALISADE follow-on], and ARTEMIS [ARC010]). The maximum peanut protein administered as a single dose during DBPCFCs was 1000 mg (PALISADE and ARTEMIS) and 2000 mg (ARC004). Symptoms were classified by system organ class (SOC) and maximum severity. Endpoints were changes in symptom severity and freedom from symptoms (ie, asymptomatic) during DBPCFC. Relative risk (RR) was calculated for symptom severity by SOC and freedom from symptoms between groups; descriptive statistics were used to summarize all other data.</p><p><strong>Results: </strong>The risk of any respiratory (RR 0.42 [0.30-0.60], P < 0.0001), gastrointestinal (RR 0.34 [0.26-0.44], P < 0.0001), cardiovascular/neurological (RR 0.17 [0.08-0.39], P < 0.001), or dermatological (RR 0.33 [0.22-0.50], P < 0.0001) symptoms was significantly lower in participants treated with PTAH versus placebo upon exposure to peanut at the end of the PALISADE trial (ie, exit DBPCFC). Compared with placebo-treated participants (23.4%), the majority (76.3%) of PTAH-treated participants had no symptoms at the exit DBPCFC when tested at the peanut protein dose not tolerated (ie, reactive dose) during the screening DBPCFC. Significantly higher proportions of PTAH-treated participants were asymptomatic at doses ≤ 100 mg in the exit DBPCFC compared with placebo-treated participants (PALISADE: 69.35% vs 12.10%, RR 5.73 [95% confidence interval (CI) 3.55-9.26]; P < 0.0001; ARTEMIS: 67.42% vs 13.95%, RR 4.83 [95% CI 2.28-10.25]; P < 0.0001); findings were similar at peanut protein doses ≤ 1000 mg (PALISADE: RR 15.56 [95% CI 5.05-47.94]; P < 0.0001; ARTEMIS: RR 34.74 [95% CI 2.19-551.03]; P < 0.0001). In ARC004, as the period of PTAH maintenance became longer, greater proportions of participants were asymptomatic at doses of peanut protein ≤ 1000 mg in the exit DBPCFC (from 37.63% after ~ 6 months of maintenance treatment [exit DBPCFC of PALISADE] to 45.54% after ~ 13 months and 58.06% after ~ 20 months of overall PTAH maintenance treatment).</p><p><strong>Conclusions: </strong>PTAH significantly reduced symptom severity due to exposure to peanut, which is clinically relevant. When exposed to peanut, participants with peanut allergy treated with PTAH rarely had moderate or severe respiratory or cardiovascular/neurological symptoms. Oral immunotherapy with PTAH appears to reduce frequency and severity of allergic reactions in individuals with peanut allergy after accidental exposure to peanut and may enable them and their families to have an improved quality of life. Trial registration ClinicalTrials.gov, NCT02635776, registered 17 December 2015, https://clinicaltrials.gov/ct2/show/NCT02635776?term=AR101&draw=2&rank=7 ; ClinicalTrials.gov, NCT02993107, registered 08 December 2016, https://clinicaltrials.gov/ct2/show/NCT02993107?term=AR101&draw=2&rank=6 ; ClinicalTrials.gov, NCT03201003, registered 22 June 2017, https://clinicaltrials.gov/ct2/show/NCT03201003 ? term = AR101&draw = 2&rank = 9.</p>","PeriodicalId":7702,"journal":{"name":"Allergy, Asthma, and Clinical Immunology : Official Journal of the Canadian Society of Allergy and Clinical Immunology","volume":"19 1","pages":"21"},"PeriodicalIF":0.0000,"publicationDate":"2023-03-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10009988/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Allergy, Asthma, and Clinical Immunology : Official Journal of the Canadian Society of Allergy and Clinical Immunology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13223-023-00757-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Peanut allergy and its current management, involving peanut avoidance and use of rescue medication during instances of accidental exposure, are burdensome to patients and their caregivers and can be a source of stress, uncertainty, and restriction. Physicians may also be frustrated with a lack of effective and safe treatments other than avoidance in the current management of peanut allergy. Efficacy, determined using double-blind, placebo-controlled food challenges (DBPCFCs), of oral immunotherapy with peanut (Arachis hypogaea) allergen powder-dnfp (PTAH; Palforzia®) was demonstrated versus placebo in children and adolescents aged 4 to 17 years in multiple phase 3 trials; continued benefit of PTAH was shown in a follow-on trial. The DBPCFC is a reproducible, rigorous, and clinically meaningful assessment accepted by regulatory authorities to evaluate the level of tolerance as an endpoint for accidental exposures to peanut in real life. It also provides useful clinical and patient-relevant information, including the amount of peanut protein an individual with peanut allergy can consume without experiencing dose-limiting symptoms, severity of symptoms, and organs affected upon ingestion of peanut protein. We explored symptoms of peanut exposure during DBPCFCs from phase 3 and follow-on trials of PTAH to further characterize treatment efficacy from a perspective relevant to patients, caregivers, and clinicians.
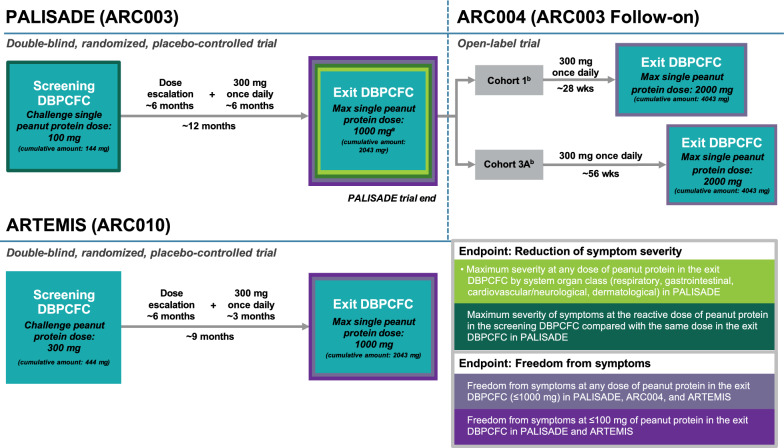
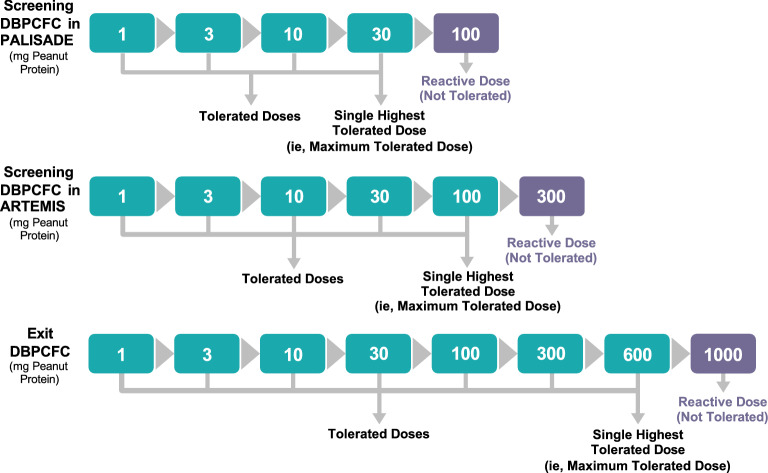
Methods: Symptom data recorded during screening and/or exit DBPCFCs from participants aged 4 to 17 years receiving PTAH or placebo were examined post hoc across three PTAH trials (PALISADE [ARC003], ARC004 [PALISADE follow-on], and ARTEMIS [ARC010]). The maximum peanut protein administered as a single dose during DBPCFCs was 1000 mg (PALISADE and ARTEMIS) and 2000 mg (ARC004). Symptoms were classified by system organ class (SOC) and maximum severity. Endpoints were changes in symptom severity and freedom from symptoms (ie, asymptomatic) during DBPCFC. Relative risk (RR) was calculated for symptom severity by SOC and freedom from symptoms between groups; descriptive statistics were used to summarize all other data.
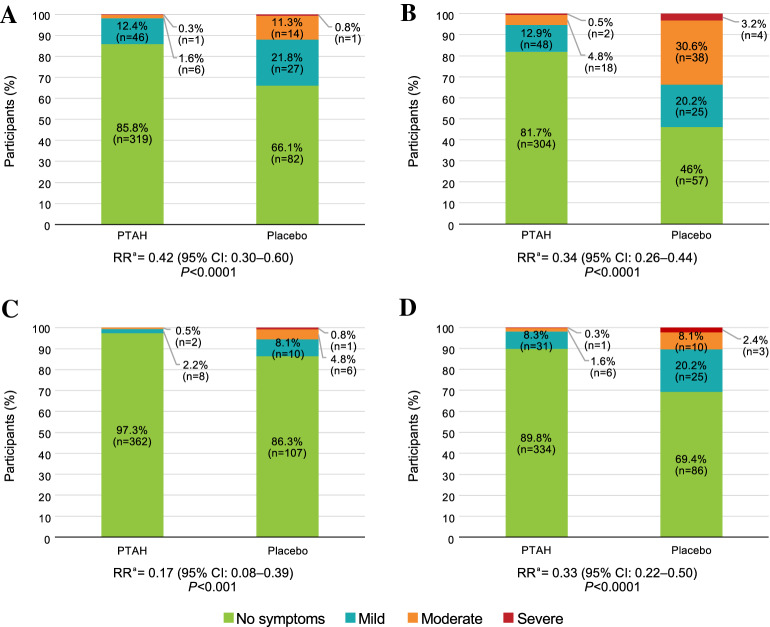
Results: The risk of any respiratory (RR 0.42 [0.30-0.60], P < 0.0001), gastrointestinal (RR 0.34 [0.26-0.44], P < 0.0001), cardiovascular/neurological (RR 0.17 [0.08-0.39], P < 0.001), or dermatological (RR 0.33 [0.22-0.50], P < 0.0001) symptoms was significantly lower in participants treated with PTAH versus placebo upon exposure to peanut at the end of the PALISADE trial (ie, exit DBPCFC). Compared with placebo-treated participants (23.4%), the majority (76.3%) of PTAH-treated participants had no symptoms at the exit DBPCFC when tested at the peanut protein dose not tolerated (ie, reactive dose) during the screening DBPCFC. Significantly higher proportions of PTAH-treated participants were asymptomatic at doses ≤ 100 mg in the exit DBPCFC compared with placebo-treated participants (PALISADE: 69.35% vs 12.10%, RR 5.73 [95% confidence interval (CI) 3.55-9.26]; P < 0.0001; ARTEMIS: 67.42% vs 13.95%, RR 4.83 [95% CI 2.28-10.25]; P < 0.0001); findings were similar at peanut protein doses ≤ 1000 mg (PALISADE: RR 15.56 [95% CI 5.05-47.94]; P < 0.0001; ARTEMIS: RR 34.74 [95% CI 2.19-551.03]; P < 0.0001). In ARC004, as the period of PTAH maintenance became longer, greater proportions of participants were asymptomatic at doses of peanut protein ≤ 1000 mg in the exit DBPCFC (from 37.63% after ~ 6 months of maintenance treatment [exit DBPCFC of PALISADE] to 45.54% after ~ 13 months and 58.06% after ~ 20 months of overall PTAH maintenance treatment).
Conclusions: PTAH significantly reduced symptom severity due to exposure to peanut, which is clinically relevant. When exposed to peanut, participants with peanut allergy treated with PTAH rarely had moderate or severe respiratory or cardiovascular/neurological symptoms. Oral immunotherapy with PTAH appears to reduce frequency and severity of allergic reactions in individuals with peanut allergy after accidental exposure to peanut and may enable them and their families to have an improved quality of life. Trial registration ClinicalTrials.gov, NCT02635776, registered 17 December 2015, https://clinicaltrials.gov/ct2/show/NCT02635776?term=AR101&draw=2&rank=7 ; ClinicalTrials.gov, NCT02993107, registered 08 December 2016, https://clinicaltrials.gov/ct2/show/NCT02993107?term=AR101&draw=2&rank=6 ; ClinicalTrials.gov, NCT03201003, registered 22 June 2017, https://clinicaltrials.gov/ct2/show/NCT03201003 ? term = AR101&draw = 2&rank = 9.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
