Effectiveness of levosimendan and role of cardiac magnetic resonance in cardiogenic shock due to COVID-19 related lymphocytic myocarditis in the course of viral sepsis.
Francesco Mangini, Elvira Bruno, Remo Caramia, Roberto Flora, Eluisa Muscogiuri, Antonio Medico, Grazia Casavecchia, Robert W W Biederman, Rinaldo Giaccari
{"title":"Effectiveness of levosimendan and role of cardiac magnetic resonance in cardiogenic shock due to COVID-19 related lymphocytic myocarditis in the course of viral sepsis.","authors":"Francesco Mangini, Elvira Bruno, Remo Caramia, Roberto Flora, Eluisa Muscogiuri, Antonio Medico, Grazia Casavecchia, Robert W W Biederman, Rinaldo Giaccari","doi":"10.22551/2023.38.1001.10236","DOIUrl":null,"url":null,"abstract":"<p><p>COVID-19 and sepsis pose great challenges to clinicians and growing evidence is demonstrating links between the two conditions. Both can be complicated by acute heart failure. The use of levosimendan in patients with ventricular dysfunction during COVID-19 infection and sepsis has very little evidence. A 46-year-old, hypertensive and obese patient was admitted for severe left ventricular failure and shock during sepsis following a COVID-19 infection. The patient was treated first with norepinephrine, which was partially effective, then with the addition of levosimendan as a continuous 24 hours infusion. Vital signs and echocardiographic systolic performance indices, such as FE, SVi, CI, dP/dT, TAPSE, and tricuspid S-wave velocity, as well as diastolic function, were recorded at access, 12 and 24 hours. After initiation of levosimendan, a rapid improvement in vital signs and systolic and diastolic performance indices was observed, not depending on changes in preload, afterload, and inflammatory status. Blood cultures were negative for the presence of bacteria, thus defining the picture of likely viral sepsis. Cardiac magnetic resonance was determinant, showing a picture of myocarditis sustained by immune processes rather than direct viral injury, which was confirmed by endomyocardial biopsy. In conclusion, this case highlights the efficacy of levosimendan in acute heart failure complicated by shock due to COVID-19-related myocarditis and concomitant sepsis and confirms cardiac magnetic resonance as the gold standard for the diagnosis of myocardial inflammatory disease. To the best of our knowledge, this is the first documented case of effective use of levosimendan in this context.</p>","PeriodicalId":72274,"journal":{"name":"Archive of clinical cases","volume":"10 1","pages":"32-38"},"PeriodicalIF":0.6000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b1/a3/acc-10-01-32.PMC10012167.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archive of clinical cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22551/2023.38.1001.10236","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
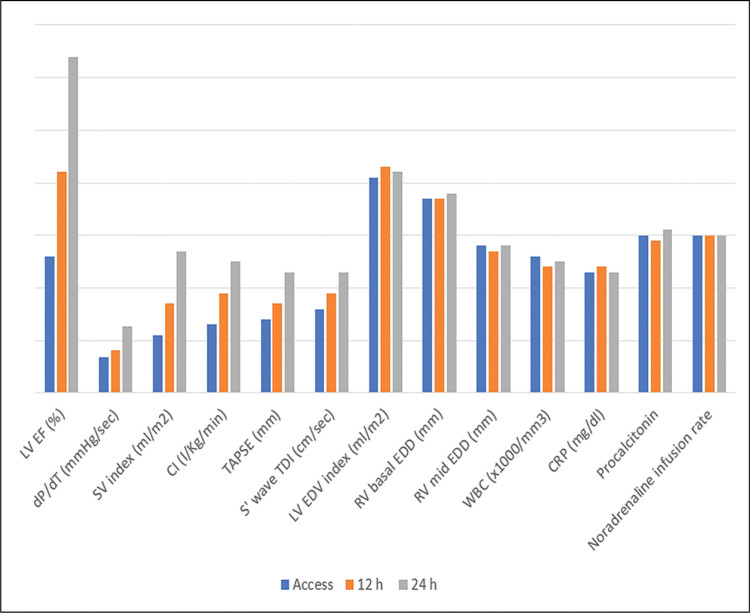
COVID-19 and sepsis pose great challenges to clinicians and growing evidence is demonstrating links between the two conditions. Both can be complicated by acute heart failure. The use of levosimendan in patients with ventricular dysfunction during COVID-19 infection and sepsis has very little evidence. A 46-year-old, hypertensive and obese patient was admitted for severe left ventricular failure and shock during sepsis following a COVID-19 infection. The patient was treated first with norepinephrine, which was partially effective, then with the addition of levosimendan as a continuous 24 hours infusion. Vital signs and echocardiographic systolic performance indices, such as FE, SVi, CI, dP/dT, TAPSE, and tricuspid S-wave velocity, as well as diastolic function, were recorded at access, 12 and 24 hours. After initiation of levosimendan, a rapid improvement in vital signs and systolic and diastolic performance indices was observed, not depending on changes in preload, afterload, and inflammatory status. Blood cultures were negative for the presence of bacteria, thus defining the picture of likely viral sepsis. Cardiac magnetic resonance was determinant, showing a picture of myocarditis sustained by immune processes rather than direct viral injury, which was confirmed by endomyocardial biopsy. In conclusion, this case highlights the efficacy of levosimendan in acute heart failure complicated by shock due to COVID-19-related myocarditis and concomitant sepsis and confirms cardiac magnetic resonance as the gold standard for the diagnosis of myocardial inflammatory disease. To the best of our knowledge, this is the first documented case of effective use of levosimendan in this context.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
