下载PDF
{"title":"Tacrolimus-associated posterior reversible encephalopathy syndrome in hematopoietic allogeneic stem cell transplantation","authors":"Aimee E. Hammerstrom, Joshua Howell, Alison Gulbis, Gabriela Rondon, Richard E. Champlin, Uday Popat","doi":"10.1002/ajh.23402","DOIUrl":null,"url":null,"abstract":"<div>\n <p>Tacrolimus-associated posterior reversible encephalopathy syndrome (PRES) is a potential complication of allogeneic stem cell transplant (SCT). Due to the paucity of information on the management of PRES in SCT patients receiving tacrolimus, more information is needed on trends associated with the incidence of PRES and to characterize its management. A retrospective review was conducted of patients receiving tacrolimus for prevention of graft versus host disease (GVHD) after allogeneic SCT who developed PRES from September 2008 to July 2011. Nineteen patients were identified. Altered mental status, seizures, and visual abnormalities were experienced by 78.9%, 52.6%, and 31.5% of the patients, respectively, at time of PRES onset. Compared with baseline, patients with PRES were likely to have an increase in mean arterial pressure (<i>P</i> < 0.0001) and serum creatinine. Elevated tacrolimus levels and hypomagnesemia were not observed with PRES onset. Tacrolimus was managed in three general strategy groups: not held, held then continued, and switched to another agent. Survival was defined as survival to discharge from PRES hospitalization. When tacrolimus was not held, held then continued, or switched to another agent, 40% (2 of 5), 40% (4/10), and 50% (2/4) survived to discharge, respectively. PRES was associated with high blood pressure and adequate blood pressure control should be part of its management. No management strategy pertaining to tacrolimus usage appeared more beneficial over another. Am. J. Hematol. 88:301–305, 2013. © 2013 Wiley Periodicals, Inc.</p>\n </div>","PeriodicalId":7724,"journal":{"name":"American Journal of Hematology","volume":"88 4","pages":"301-305"},"PeriodicalIF":9.9000,"publicationDate":"2013-02-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/ajh.23402","citationCount":"79","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Hematology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ajh.23402","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 79
引用
批量引用
Abstract
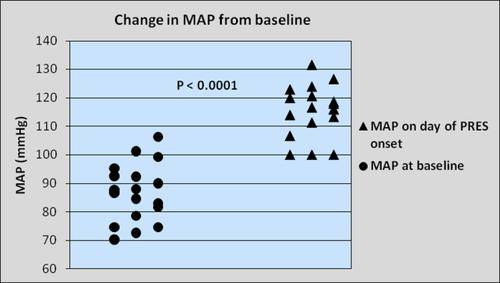
Tacrolimus-associated posterior reversible encephalopathy syndrome (PRES) is a potential complication of allogeneic stem cell transplant (SCT). Due to the paucity of information on the management of PRES in SCT patients receiving tacrolimus, more information is needed on trends associated with the incidence of PRES and to characterize its management. A retrospective review was conducted of patients receiving tacrolimus for prevention of graft versus host disease (GVHD) after allogeneic SCT who developed PRES from September 2008 to July 2011. Nineteen patients were identified. Altered mental status, seizures, and visual abnormalities were experienced by 78.9%, 52.6%, and 31.5% of the patients, respectively, at time of PRES onset. Compared with baseline, patients with PRES were likely to have an increase in mean arterial pressure (P < 0.0001) and serum creatinine. Elevated tacrolimus levels and hypomagnesemia were not observed with PRES onset. Tacrolimus was managed in three general strategy groups: not held, held then continued, and switched to another agent. Survival was defined as survival to discharge from PRES hospitalization. When tacrolimus was not held, held then continued, or switched to another agent, 40% (2 of 5), 40% (4/10), and 50% (2/4) survived to discharge, respectively. PRES was associated with high blood pressure and adequate blood pressure control should be part of its management. No management strategy pertaining to tacrolimus usage appeared more beneficial over another. Am. J. Hematol. 88:301–305, 2013. © 2013 Wiley Periodicals, Inc.
异基因造血干细胞移植中他克莫司相关的后部可逆性脑病综合征
他克莫司相关的后部可逆性脑病综合征(PRES)是同种异体干细胞移植(SCT)的潜在并发症。由于对接受他克莫司治疗的SCT患者的PRES管理信息的缺乏,需要更多的信息来了解PRES发病率的相关趋势及其管理特征。对2008年9月至2011年7月间发生PRES的同种异体SCT术后接受他克莫司预防移植物抗宿主病(GVHD)的患者进行了回顾性研究。确认了19例患者。在PRES发病时,78.9%、52.6%和31.5%的患者分别出现精神状态改变、癫痫发作和视觉异常。与基线相比,PRES患者的平均动脉压可能增加(P <0.0001)和血清肌酐。PRES发病时未观察到他克莫司水平升高和低镁血症。他克莫司分为三个一般策略组:不持有,持有后继续服用,然后切换到另一种药物。生存期定义为从PRES住院出院的生存期。当不服用他克莫司、继续服用他克莫司或改用其他药物时,分别有40%(2/ 5)、40%(4/10)和50%(2/4)存活至出院。press与高血压有关,适当的血压控制应是其管理的一部分。没有一种与他克莫司使用有关的管理策略比另一种更有益。点。中华血液学杂志,2013,33(4):391 - 391。©2013 Wiley期刊公司
本文章由计算机程序翻译,如有差异,请以英文原文为准。


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
