Yong-Hao Pua, Laura Tay, Ross Allan Clark, Julian Thumboo, Ee-Ling Tay, Shi-Min Mah, Pei-Yueng Lee, Yee-Sien Ng
{"title":"Development and validation of a physical frailty phenotype index-based model to estimate the frailty index.","authors":"Yong-Hao Pua, Laura Tay, Ross Allan Clark, Julian Thumboo, Ee-Ling Tay, Shi-Min Mah, Pei-Yueng Lee, Yee-Sien Ng","doi":"10.1186/s41512-023-00143-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The conventional count-based physical frailty phenotype (PFP) dichotomizes its criterion predictors-an approach that creates information loss and depends on the availability of population-derived cut-points. This study proposes an alternative approach to computing the PFP by developing and validating a model that uses PFP components to predict the frailty index (FI) in community-dwelling older adults, without the need for predictor dichotomization.</p><p><strong>Methods: </strong>A sample of 998 community-dwelling older adults (mean [SD], 68 [7] years) participated in this prospective cohort study. Participants completed a multi-domain geriatric screen and a physical fitness assessment from which the count-based PFP and the 36-item FI were computed. One-year prospective falls and hospitalization rates were also measured. Bayesian beta regression analysis, allowing for nonlinear effects of the non-dichotomized PFP criterion predictors, was used to develop a model for FI (\"model-based PFP\"). Approximate leave-one-out (LOO) cross-validation was used to examine model overfitting.</p><p><strong>Results: </strong>The model-based PFP showed good calibration with the FI, and it had better out-of-sample predictive performance than the count-based PFP (LOO-R<sup>2</sup>, 0.35 vs 0.22). In clinical terms, the improvement in prediction (i) translated to improved classification agreement with the FI (Cohen's k<sub>w</sub>, 0.47 vs 0.36) and (ii) resulted primarily in a 23% (95%CI, 18-28%) net increase in FI-defined \"prefrail/frail\" participants correctly classified. The model-based PFP showed stronger prognostic performance for predicting falls and hospitalization than did the count-based PFP.</p><p><strong>Conclusion: </strong>The developed model-based PFP predicted FI and clinical outcomes more strongly than did the count-based PFP in community-dwelling older adults. By not requiring predictor cut-points, the model-based PFP potentially facilitates usage and feasibility. Future validation studies should aim to obtain clear evidence on the benefits of this approach.</p>","PeriodicalId":72800,"journal":{"name":"Diagnostic and prognostic research","volume":"7 1","pages":"5"},"PeriodicalIF":2.6000,"publicationDate":"2023-03-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10029224/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diagnostic and prognostic research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41512-023-00143-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The conventional count-based physical frailty phenotype (PFP) dichotomizes its criterion predictors-an approach that creates information loss and depends on the availability of population-derived cut-points. This study proposes an alternative approach to computing the PFP by developing and validating a model that uses PFP components to predict the frailty index (FI) in community-dwelling older adults, without the need for predictor dichotomization.
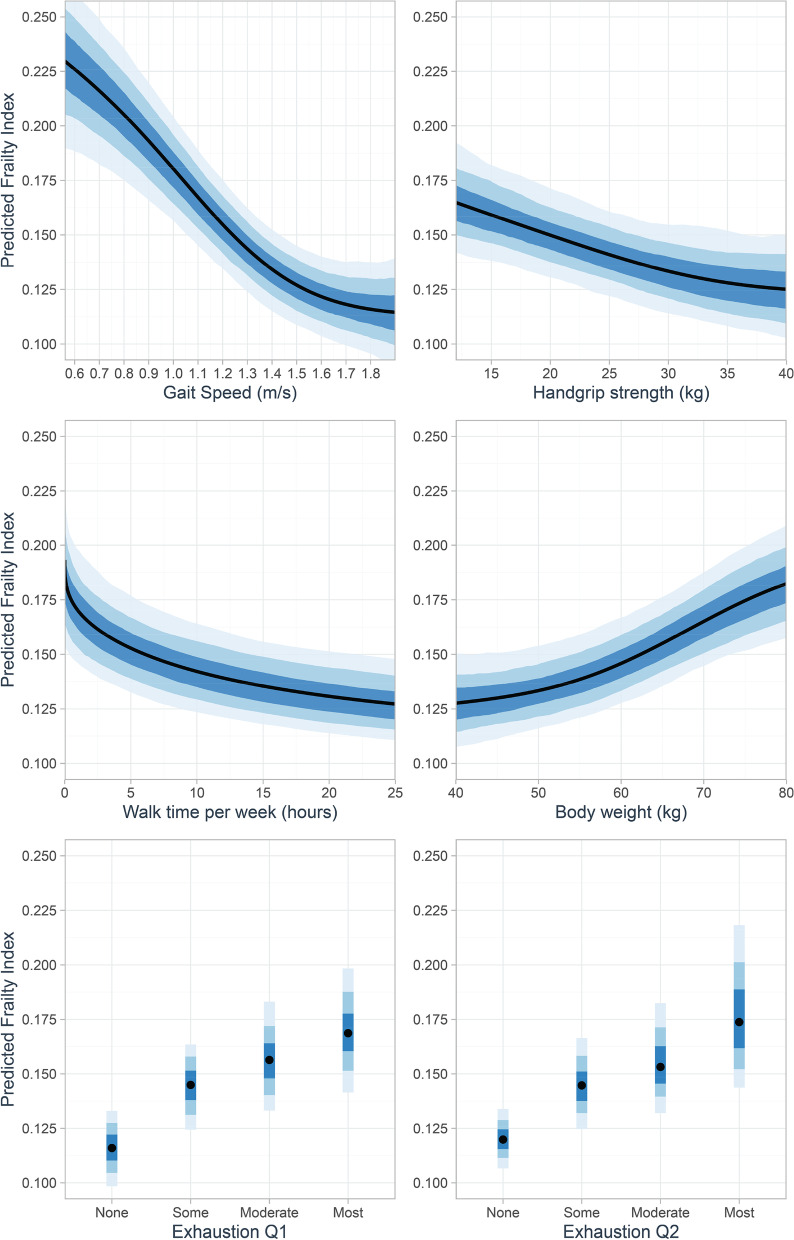
Methods: A sample of 998 community-dwelling older adults (mean [SD], 68 [7] years) participated in this prospective cohort study. Participants completed a multi-domain geriatric screen and a physical fitness assessment from which the count-based PFP and the 36-item FI were computed. One-year prospective falls and hospitalization rates were also measured. Bayesian beta regression analysis, allowing for nonlinear effects of the non-dichotomized PFP criterion predictors, was used to develop a model for FI ("model-based PFP"). Approximate leave-one-out (LOO) cross-validation was used to examine model overfitting.
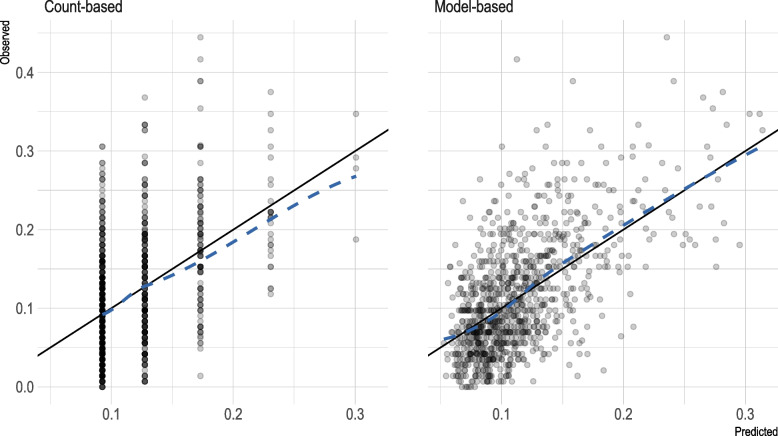
Results: The model-based PFP showed good calibration with the FI, and it had better out-of-sample predictive performance than the count-based PFP (LOO-R2, 0.35 vs 0.22). In clinical terms, the improvement in prediction (i) translated to improved classification agreement with the FI (Cohen's kw, 0.47 vs 0.36) and (ii) resulted primarily in a 23% (95%CI, 18-28%) net increase in FI-defined "prefrail/frail" participants correctly classified. The model-based PFP showed stronger prognostic performance for predicting falls and hospitalization than did the count-based PFP.
Conclusion: The developed model-based PFP predicted FI and clinical outcomes more strongly than did the count-based PFP in community-dwelling older adults. By not requiring predictor cut-points, the model-based PFP potentially facilitates usage and feasibility. Future validation studies should aim to obtain clear evidence on the benefits of this approach.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
