Davide Restelli, Olimpia Trio, Cristina Poleggi, Maurizio Cusmà Piccione, Roberta Manganaro, Giuseppe Certo, Concetta Zito, Giuseppe Andò
{"title":"Nonbacterial Thrombotic Endocarditis with Atypical Presentation as Overt Congestive Heart Failure.","authors":"Davide Restelli, Olimpia Trio, Cristina Poleggi, Maurizio Cusmà Piccione, Roberta Manganaro, Giuseppe Certo, Concetta Zito, Giuseppe Andò","doi":"10.4103/jcecho.jcecho_42_22","DOIUrl":null,"url":null,"abstract":"<p><p>Nonbacterial thrombotic endocarditis (NBTE) is a form of endocarditis associated with malignancy or autoimmune disorders. Diagnosis remains a challenge as patients are often asymptomatic up to embolic events or rarely, valve dysfunction. We report a case of NBTE with uncommon clinical presentation and identified with multimodal echocardiography. An 82-year-old man presented to our outpatient clinic reporting dyspnea. Past medical history included hypertension, diabetes, kidney disease, and unprovoked deep-vein thrombosis. On physical examination, he was apyretic, mildly hypotensive, and hypoxemic, had a systolic murmur and lower limbs edema. Transthoracic echocardiography revealed severe mitral regurgitation due to verrucous thickening of the free margin of both leaflets, increased pulmonary pressure, and dilated inferior vena cava. Multiple blood cultures were negative. Transesophageal echocardiography confirmed \"thrombotic\" thickening of mitral leaflets. Nuclear investigations were highly suggestive of multi-metastatic pulmonary cancer. We did not further proceed with the diagnostic workup and prescribed palliative care. Lesions seen on echocardiography were suggestive of NBTE: they involved both sides of mitral leaflets, close to the edges, had irregular shape and echo density, a broad base, and no independent motion. Criteria for infective endocarditis were not met and the final diagnosis was paraneoplastic NBTE due to underlying lung cancer. We remark the lack of definitive recommendations about the treatment of NBTE and the only role of anticoagulation to prevent systemic embolism. We have reported a case of NBTE presenting with atypical symptoms and likely related to the prothrombotic state induced by underlying lung cancer. Provided the unconclusive microbiological tests, multimodal imaging has played a crucial role in the final diagnosis.</p>","PeriodicalId":15191,"journal":{"name":"Journal of Cardiovascular Echography","volume":"32 4","pages":"225-228"},"PeriodicalIF":1.0000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10041397/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Echography","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jcecho.jcecho_42_22","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/23 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
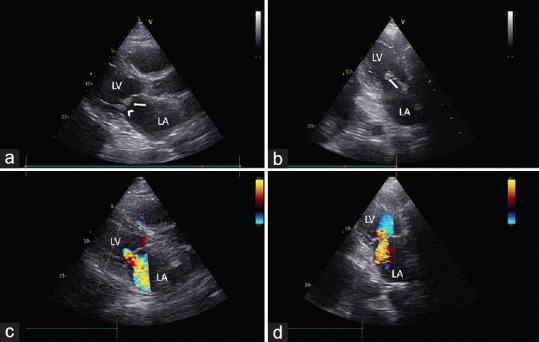
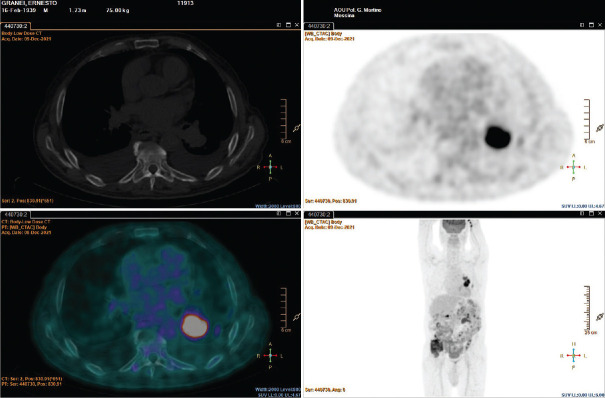
Nonbacterial thrombotic endocarditis (NBTE) is a form of endocarditis associated with malignancy or autoimmune disorders. Diagnosis remains a challenge as patients are often asymptomatic up to embolic events or rarely, valve dysfunction. We report a case of NBTE with uncommon clinical presentation and identified with multimodal echocardiography. An 82-year-old man presented to our outpatient clinic reporting dyspnea. Past medical history included hypertension, diabetes, kidney disease, and unprovoked deep-vein thrombosis. On physical examination, he was apyretic, mildly hypotensive, and hypoxemic, had a systolic murmur and lower limbs edema. Transthoracic echocardiography revealed severe mitral regurgitation due to verrucous thickening of the free margin of both leaflets, increased pulmonary pressure, and dilated inferior vena cava. Multiple blood cultures were negative. Transesophageal echocardiography confirmed "thrombotic" thickening of mitral leaflets. Nuclear investigations were highly suggestive of multi-metastatic pulmonary cancer. We did not further proceed with the diagnostic workup and prescribed palliative care. Lesions seen on echocardiography were suggestive of NBTE: they involved both sides of mitral leaflets, close to the edges, had irregular shape and echo density, a broad base, and no independent motion. Criteria for infective endocarditis were not met and the final diagnosis was paraneoplastic NBTE due to underlying lung cancer. We remark the lack of definitive recommendations about the treatment of NBTE and the only role of anticoagulation to prevent systemic embolism. We have reported a case of NBTE presenting with atypical symptoms and likely related to the prothrombotic state induced by underlying lung cancer. Provided the unconclusive microbiological tests, multimodal imaging has played a crucial role in the final diagnosis.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
