Pedro Pimentel-Nunes, Raquel Ortigão, Luís Pedro Afonso, Rui Pedro Bastos, Diogo Libânio, Mário Dinis-Ribeiro
{"title":"Endoscopic Resection of Gastrointestinal Neuroendocrine Tumors: Long-Term Outcomes and Comparison of Endoscopic Techniques.","authors":"Pedro Pimentel-Nunes, Raquel Ortigão, Luís Pedro Afonso, Rui Pedro Bastos, Diogo Libânio, Mário Dinis-Ribeiro","doi":"10.1159/000521654","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Gastrointestinal neuroendocrine tumors (GI-NETs) are being more frequently diagnosed and treated by endoscopic resection (ER) techniques. However, comparison studies of the different ER techniques or long-term outcomes are rarely reported.</p><p><strong>Methods: </strong>This was a single-center retrospective study analyzing short and long-term outcomes after ER of gastric, duodenum, and rectal GI-NETs. Comparison between standard EMR (sEMR), EMR with a cap (EMRc), and endoscopic submucosal dissection (ESD) was made.</p><p><strong>Results: </strong>Fifty-three patients with GI-NET (25 gastric, 15 duodenal, and 13 rectal; sEMR = 21; EMRc = 19; ESD = 13) were included in the analysis. Median tumor size was 11 mm (range 4-20), significantly larger in the ESD and EMRc groups compared to the sEMR group (<i>p</i> < 0.05). Complete ER was possible in all cases with 68% histological complete resection (no difference between the groups). Complication rate was significantly higher in the EMRc group (EMRc 32%, ESD 8%, and EMRs 0%, p = 0.01). Local recurrence occurred in only one patient, and systemic recurrence in 6%, with size ≥ 12 mm being a risk factor for systemic recurrence (p = 0.05). Specific disease-free survival after ER was 98%.</p><p><strong>Conclusion: </strong>ER is a safe and highly effective treatment particularly for less than 12 mm luminal GI-NETs. EMRc is associated with a high complication rate and should be avoided. sEMR is an easy and safe technique that is associated with long-term curability, and it is probably the best therapeutic option for most luminal GI-NETs. ESD appears to be the best option for lesions that cannot be resected en bloc with sEMR. Multicenter, prospective randomized trials should confirm these results.</p>","PeriodicalId":51838,"journal":{"name":"GE Portuguese Journal of Gastroenterology","volume":"30 2","pages":"98-106"},"PeriodicalIF":0.6000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f4/e1/pjg-0030-0098.PMC10050860.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"GE Portuguese Journal of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000521654","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 2
Abstract
Introduction: Gastrointestinal neuroendocrine tumors (GI-NETs) are being more frequently diagnosed and treated by endoscopic resection (ER) techniques. However, comparison studies of the different ER techniques or long-term outcomes are rarely reported.
Methods: This was a single-center retrospective study analyzing short and long-term outcomes after ER of gastric, duodenum, and rectal GI-NETs. Comparison between standard EMR (sEMR), EMR with a cap (EMRc), and endoscopic submucosal dissection (ESD) was made.
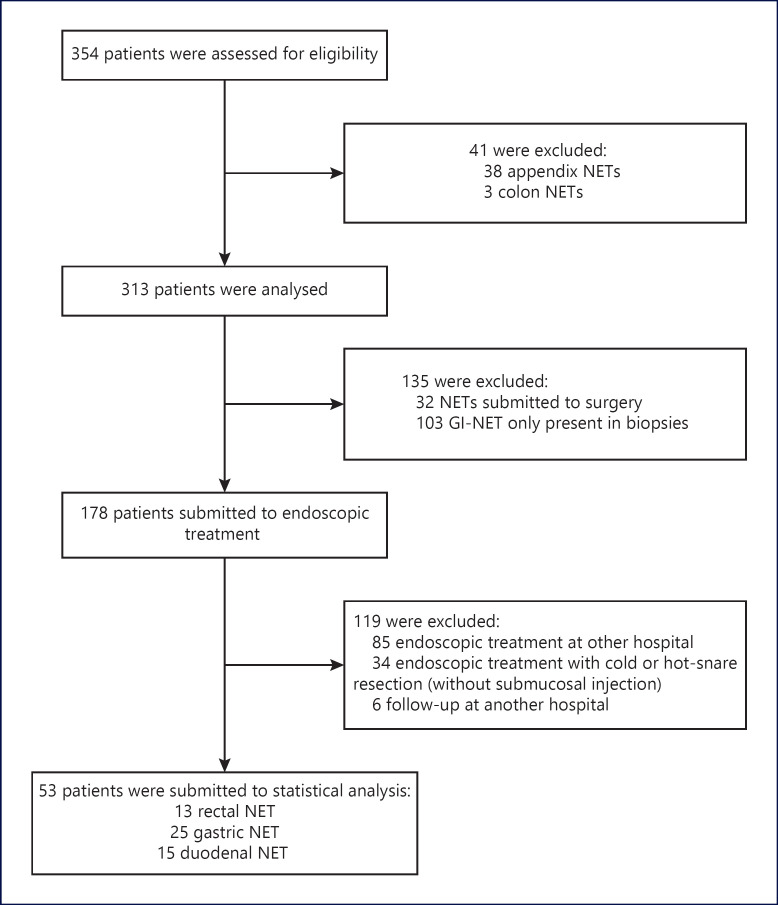
Results: Fifty-three patients with GI-NET (25 gastric, 15 duodenal, and 13 rectal; sEMR = 21; EMRc = 19; ESD = 13) were included in the analysis. Median tumor size was 11 mm (range 4-20), significantly larger in the ESD and EMRc groups compared to the sEMR group (p < 0.05). Complete ER was possible in all cases with 68% histological complete resection (no difference between the groups). Complication rate was significantly higher in the EMRc group (EMRc 32%, ESD 8%, and EMRs 0%, p = 0.01). Local recurrence occurred in only one patient, and systemic recurrence in 6%, with size ≥ 12 mm being a risk factor for systemic recurrence (p = 0.05). Specific disease-free survival after ER was 98%.
Conclusion: ER is a safe and highly effective treatment particularly for less than 12 mm luminal GI-NETs. EMRc is associated with a high complication rate and should be avoided. sEMR is an easy and safe technique that is associated with long-term curability, and it is probably the best therapeutic option for most luminal GI-NETs. ESD appears to be the best option for lesions that cannot be resected en bloc with sEMR. Multicenter, prospective randomized trials should confirm these results.
期刊介绍:
The ''GE Portuguese Journal of Gastroenterology'' (formerly Jornal Português de Gastrenterologia), founded in 1994, is the official publication of Sociedade Portuguesa de Gastrenterologia (Portuguese Society of Gastroenterology), Sociedade Portuguesa de Endoscopia Digestiva (Portuguese Society of Digestive Endoscopy) and Associação Portuguesa para o Estudo do Fígado (Portuguese Association for the Study of the Liver). The journal publishes clinical and basic research articles on Gastroenterology, Digestive Endoscopy, Hepatology and related topics. Review articles, clinical case studies, images, letters to the editor and other articles such as recommendations or papers on gastroenterology clinical practice are also considered. Only articles written in English are accepted.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
