Mohammad Abuqbeitah, Mustafa Demir, Sağit Sağer, Sertaç Asa, Nazenin Ipek Işıkcı, Kerim Sönmezoğlu
{"title":"SPECT/CT-based dosimetry of salivary glands and iodine-avid lesions following <sup>131</sup>I therapy.","authors":"Mohammad Abuqbeitah, Mustafa Demir, Sağit Sağer, Sertaç Asa, Nazenin Ipek Işıkcı, Kerim Sönmezoğlu","doi":"10.1007/s12553-022-00718-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The purpose was to provide uptake and radiation dose estimates to salivary glands (SG) and pathologic lesions following radioiodine therapy (RIT) of differentiated thyroid cancer patients (DTC).</p><p><strong>Methods: </strong>A group of DTC patients (n = 25) undergoing <sup>131</sup>I therapy joined this study with varying amounts of therapeutic activity. Sequential SPECT/CT scans were acquired at 4 ± 2, 24 ± 2, and 168 ± 3 h following administration of 3497-9250 MBq 131I. An earlier experiment with Acrylic glass body phantom (PET Phantom NEMA 2012 / IEC 2008) was conducted for system calibration including scatter, partial volume effect and count loss correction. Dose calculation was made via IDAC-Dose 2.1 code.</p><p><strong>Results: </strong>The absorbed dose to parotid glands was 0.04-0.97 Gy/GBq (median: 0.26 Gy/GBq). The median absorbed dose to submandibular glands was 0.14 Gy/GBq (0.05 to 0.56 Gy/GBq). The absorbed dose to thyroid residues was from 0.55 to 399.5 Gy/GBq (median: 21.8 Gy/GBq), and that to distal lesions ranged from 0.78 to 28.0 Gy/GBq (median: 3.12 Gy/GBq). 41% of the thyroid residues received dose > 80 Gy, 18% between 70-80 Gy, 18% between 40-70 Gy, and 23% has dose < 40 Gy. In contrast, 18% of the metastases exhibited a dose > 80 Gy, 9% between 40-60 Gy, and the dose to the vast majority of lesions (64%) was < 40 Gy.</p><p><strong>Conclusion: </strong>It was inferred that dose estimation after RIT with SPECT/CT is feasible to apply, together with good agreement with published <sup>124</sup>I PET/CT dose estimates. A broad and sub-effective dose range was estimated for thyroid residues and distal lesions. Moreover, the current methodology might be useful for establishing a dose-effect relationship and radiation-induced salivary glands damage after RIT.</p>","PeriodicalId":12941,"journal":{"name":"Health and Technology","volume":"13 1","pages":"101-110"},"PeriodicalIF":2.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9817440/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health and Technology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s12553-022-00718-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICAL INFORMATICS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The purpose was to provide uptake and radiation dose estimates to salivary glands (SG) and pathologic lesions following radioiodine therapy (RIT) of differentiated thyroid cancer patients (DTC).
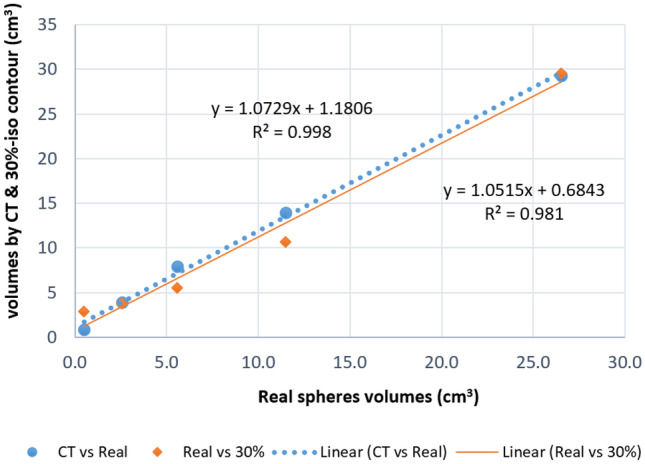
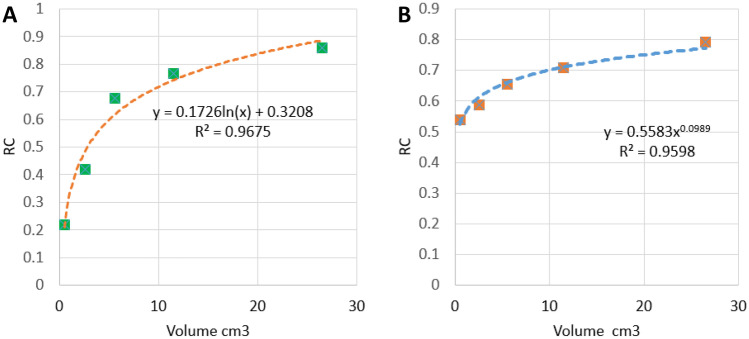
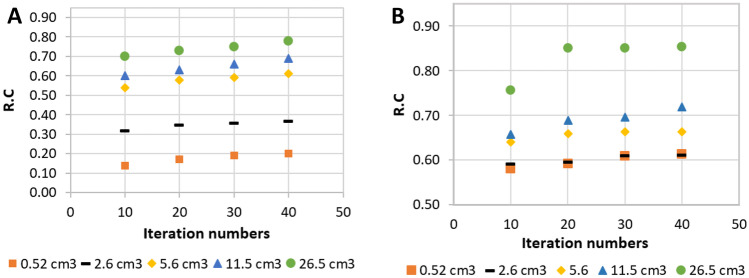
Methods: A group of DTC patients (n = 25) undergoing 131I therapy joined this study with varying amounts of therapeutic activity. Sequential SPECT/CT scans were acquired at 4 ± 2, 24 ± 2, and 168 ± 3 h following administration of 3497-9250 MBq 131I. An earlier experiment with Acrylic glass body phantom (PET Phantom NEMA 2012 / IEC 2008) was conducted for system calibration including scatter, partial volume effect and count loss correction. Dose calculation was made via IDAC-Dose 2.1 code.
Results: The absorbed dose to parotid glands was 0.04-0.97 Gy/GBq (median: 0.26 Gy/GBq). The median absorbed dose to submandibular glands was 0.14 Gy/GBq (0.05 to 0.56 Gy/GBq). The absorbed dose to thyroid residues was from 0.55 to 399.5 Gy/GBq (median: 21.8 Gy/GBq), and that to distal lesions ranged from 0.78 to 28.0 Gy/GBq (median: 3.12 Gy/GBq). 41% of the thyroid residues received dose > 80 Gy, 18% between 70-80 Gy, 18% between 40-70 Gy, and 23% has dose < 40 Gy. In contrast, 18% of the metastases exhibited a dose > 80 Gy, 9% between 40-60 Gy, and the dose to the vast majority of lesions (64%) was < 40 Gy.
Conclusion: It was inferred that dose estimation after RIT with SPECT/CT is feasible to apply, together with good agreement with published 124I PET/CT dose estimates. A broad and sub-effective dose range was estimated for thyroid residues and distal lesions. Moreover, the current methodology might be useful for establishing a dose-effect relationship and radiation-induced salivary glands damage after RIT.
期刊介绍:
Health and Technology is the first truly cross-disciplinary journal on issues related to health technologies addressing all professions relating to health, care and health technology.The journal constitutes an information platform connecting medical technology and informatics with the needs of care, health care professionals and patients. Thus, medical physicists and biomedical/clinical engineers are encouraged to write articles not only for their colleagues, but directed to all other groups of readers as well, and vice versa.By its nature, the journal presents and discusses hot subjects including but not limited to patient safety, patient empowerment, disease surveillance and management, e-health and issues concerning data security, privacy, reliability and management, data mining and knowledge exchange as well as health prevention. The journal also addresses the medical, financial, social, educational and safety aspects of health technologies as well as health technology assessment and management, including issues such security, efficacy, cost in comparison to the benefit, as well as social, legal and ethical implications.This journal is a communicative source for the health work force (physicians, nurses, medical physicists, clinical engineers, biomedical engineers, hospital engineers, etc.), the ministries of health, hospital management, self-employed doctors, health care providers and regulatory agencies, the medical technology industry, patients'' associations, universities (biomedical and clinical engineering, medical physics, medical informatics, biology, medicine and public health as well as health economics programs), research institutes and professional, scientific and technical organizations.Health and Technology is jointly published by Springer and the IUPESM (International Union for Physical and Engineering Sciences in Medicine) in cooperation with the World Health Organization.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
