Marcus A Florez, Brian De, Bhavana V Chapman, Anussara Prayongrat, Jonathan G Thomas, Thomas H Beckham, Chenyang Wang, Debra N Yeboa, Andrew J Bishop, Tina Briere, Behrang Amini, Jing Li, Claudio E Tatsui, Laurence D Rhines, Amol J Ghia
{"title":"Safety and efficacy of salvage conventional re-irradiation following stereotactic radiosurgery for spine metastases.","authors":"Marcus A Florez, Brian De, Bhavana V Chapman, Anussara Prayongrat, Jonathan G Thomas, Thomas H Beckham, Chenyang Wang, Debra N Yeboa, Andrew J Bishop, Tina Briere, Behrang Amini, Jing Li, Claudio E Tatsui, Laurence D Rhines, Amol J Ghia","doi":"10.3857/roj.2022.00353","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>There has been limited work assessing the use of re-irradiation (re-RT) for local failure following stereotactic spinal radiosurgery (SSRS). We reviewed our institutional experience of conventionally-fractionated external beam radiation (cEBRT) for salvage therapy following SSRS local failure.</p><p><strong>Materials and methods: </strong>We performed a retrospective review of 54 patients that underwent salvage conventional re-RT at previously SSRS-treated sites. Local control following re-RT was defined as the absence of progression at the treated site as determined by magnetic resonance imaging.</p><p><strong>Results: </strong>Competing risk analysis for local failure was performed using a Fine-Gray model. The median follow-up time was 25 months and median overall survival (OS) was 16 months (95% confidence interval [CI], 10.8-24.9 months) following cEBRT re-RT. Multivariable Cox proportional-hazards analysis revealed Karnofsky performance score prior to re-RT (hazard ratio [HR] = 0.95; 95% CI, 0.93-0.98; p = 0.003) and time to local failure (HR = 0.97; 95% CI, 0.94-1.00; p = 0.04) were associated with longer OS, while male sex (HR = 3.92; 95% CI, 1.64-9.33; p = 0.002) was associated with shorter OS. Local control at 12 months was 81% (95% CI, 69.3-94.0). Competing risk multivariable regression revealed radioresistant tumors (subhazard ratio [subHR] = 0.36; 95% CI, 0.15-0.90; p = 0.028) and epidural disease (subHR = 0.31; 95% CI, 0.12-0.78; p =0.013) were associated with increased risk of local failure. At 12 months, 91% of patients maintained ambulatory function.</p><p><strong>Conclusion: </strong>Our data suggest that cEBRT following SSRS local failure can be used safely and effectively. Further investigation is needed into optimal patient selection for cEBRT in the retreatment setting.</p>","PeriodicalId":46572,"journal":{"name":"Radiation Oncology Journal","volume":"41 1","pages":"12-22"},"PeriodicalIF":2.2000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0a/58/roj-2022-00353.PMC10073838.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation Oncology Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3857/roj.2022.00353","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
Purpose: There has been limited work assessing the use of re-irradiation (re-RT) for local failure following stereotactic spinal radiosurgery (SSRS). We reviewed our institutional experience of conventionally-fractionated external beam radiation (cEBRT) for salvage therapy following SSRS local failure.
Materials and methods: We performed a retrospective review of 54 patients that underwent salvage conventional re-RT at previously SSRS-treated sites. Local control following re-RT was defined as the absence of progression at the treated site as determined by magnetic resonance imaging.
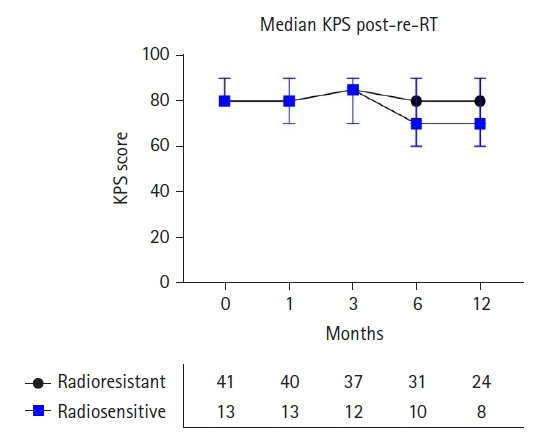
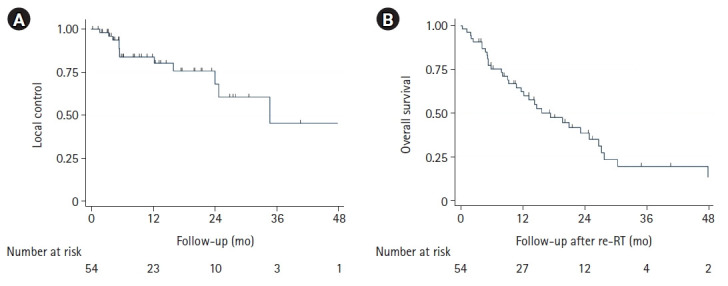
Results: Competing risk analysis for local failure was performed using a Fine-Gray model. The median follow-up time was 25 months and median overall survival (OS) was 16 months (95% confidence interval [CI], 10.8-24.9 months) following cEBRT re-RT. Multivariable Cox proportional-hazards analysis revealed Karnofsky performance score prior to re-RT (hazard ratio [HR] = 0.95; 95% CI, 0.93-0.98; p = 0.003) and time to local failure (HR = 0.97; 95% CI, 0.94-1.00; p = 0.04) were associated with longer OS, while male sex (HR = 3.92; 95% CI, 1.64-9.33; p = 0.002) was associated with shorter OS. Local control at 12 months was 81% (95% CI, 69.3-94.0). Competing risk multivariable regression revealed radioresistant tumors (subhazard ratio [subHR] = 0.36; 95% CI, 0.15-0.90; p = 0.028) and epidural disease (subHR = 0.31; 95% CI, 0.12-0.78; p =0.013) were associated with increased risk of local failure. At 12 months, 91% of patients maintained ambulatory function.
Conclusion: Our data suggest that cEBRT following SSRS local failure can be used safely and effectively. Further investigation is needed into optimal patient selection for cEBRT in the retreatment setting.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
