A Small Increase in Serum Creatinine within 48 h of Hospital Admission Is an Independent Predictor of In-Hospital Adverse Outcomes in Patients with ST-Segment Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention: Findings from the Improving Care for Cardiovascular Disease in the China Project.
{"title":"A Small Increase in Serum Creatinine within 48 h of Hospital Admission Is an Independent Predictor of In-Hospital Adverse Outcomes in Patients with ST-Segment Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention: Findings from the Improving Care for Cardiovascular Disease in the China Project.","authors":"Jiajia Zhu, Wenxian Liu, Jiang Li, Changsheng Ma, Dong Zhao","doi":"10.1155/2023/1374206","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute kidney injury (AKI) is a common complication of percutaneous coronary intervention (PCI) that has been associated with high morbidity and mortality in patients with STEMI. Acute tubular damage may be reflected by serum creatinine (Scr) values that do not meet the criteria for AKI.</p><p><strong>Methods: </strong>This analysis included 19,424 patients from the Improving Care for Cardiovascular Disease in China, Acute Coronary Syndrome Project (<i>n</i> = 5,221 (36.8%), patients with a small increase in Scr within 48 h of hospitalization; <i>n</i> = 14,203 patients with no increase in Scr). The primary outcome was the incidence of major adverse cardiovascular events (MACE). Secondary outcomes included the incidence of massive hemorrhage, in-hospital death, atrial fibrillation, heart failure, cardiogenic shock, cardiac arrest, and stroke. Logistic regression analysis was used to evaluate associations between a small increase in Scr within 48 h of hospitalization (>0.1 to <0.3 mg/dl) and MACE or massive hemorrhage during hospitalization.</p><p><strong>Results: </strong>Patients with a small increase in Scr within 48 h of hospitalization were significantly more likely to experience MACE (11.2% vs. 9.1%; <i>P</i> < 0.001) or massive hemorrhage (3.2% vs. 2.2%; <i>P</i> < 0.001) compared to patients with no increase in Scr, but there was no significant difference in in-hospital mortality (0.8% vs. 0.9%; <i>P</i>=0.301). Logistic regression analysis showed that a small increase in Scr within 48 h of hospital admission was a risk factor for MACE (OR, 1.168; 95% CI, 1.044-1.306; <i>P</i>=0.006) or massive hemorrhage (OR, 1.413; 95% CI, 1.164-1.715; <i>P</i> < 0.001). Other risk factors included age ˃65 years, history of heart failure, use of glycoprotein IIb/IIIa inhibitors, aspirin or ACEI/ARB, LVEF <40%, Killip class III-IV, and increased SBP and heart rate.</p><p><strong>Conclusion: </strong>A small increase in Scr during hospitalization in patients with STEMI undergoing primary PCI that does not meet the criteria for AKI is a risk factor for in-hospital adverse outcomes. This effect is maintained in patients with normal Scr at hospitalization. <i>Trial Registration</i>. Clinical trial registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT02306616.</p>","PeriodicalId":9494,"journal":{"name":"Cardiology Research and Practice","volume":"2023 ","pages":"1374206"},"PeriodicalIF":1.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10072956/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology Research and Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2023/1374206","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Acute kidney injury (AKI) is a common complication of percutaneous coronary intervention (PCI) that has been associated with high morbidity and mortality in patients with STEMI. Acute tubular damage may be reflected by serum creatinine (Scr) values that do not meet the criteria for AKI.
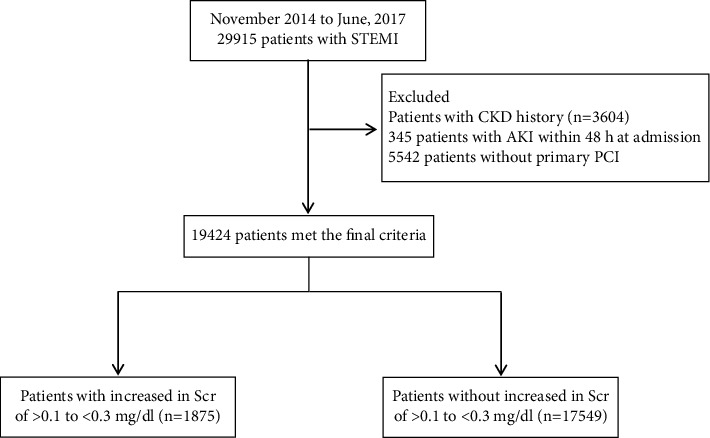
Methods: This analysis included 19,424 patients from the Improving Care for Cardiovascular Disease in China, Acute Coronary Syndrome Project (n = 5,221 (36.8%), patients with a small increase in Scr within 48 h of hospitalization; n = 14,203 patients with no increase in Scr). The primary outcome was the incidence of major adverse cardiovascular events (MACE). Secondary outcomes included the incidence of massive hemorrhage, in-hospital death, atrial fibrillation, heart failure, cardiogenic shock, cardiac arrest, and stroke. Logistic regression analysis was used to evaluate associations between a small increase in Scr within 48 h of hospitalization (>0.1 to <0.3 mg/dl) and MACE or massive hemorrhage during hospitalization.
Results: Patients with a small increase in Scr within 48 h of hospitalization were significantly more likely to experience MACE (11.2% vs. 9.1%; P < 0.001) or massive hemorrhage (3.2% vs. 2.2%; P < 0.001) compared to patients with no increase in Scr, but there was no significant difference in in-hospital mortality (0.8% vs. 0.9%; P=0.301). Logistic regression analysis showed that a small increase in Scr within 48 h of hospital admission was a risk factor for MACE (OR, 1.168; 95% CI, 1.044-1.306; P=0.006) or massive hemorrhage (OR, 1.413; 95% CI, 1.164-1.715; P < 0.001). Other risk factors included age ˃65 years, history of heart failure, use of glycoprotein IIb/IIIa inhibitors, aspirin or ACEI/ARB, LVEF <40%, Killip class III-IV, and increased SBP and heart rate.
Conclusion: A small increase in Scr during hospitalization in patients with STEMI undergoing primary PCI that does not meet the criteria for AKI is a risk factor for in-hospital adverse outcomes. This effect is maintained in patients with normal Scr at hospitalization. Trial Registration. Clinical trial registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT02306616.
期刊介绍:
Cardiology Research and Practice is a peer-reviewed, Open Access journal that publishes original research articles, review articles, and clinical studies that focus on the diagnosis and treatment of cardiovascular disease. The journal welcomes submissions related to systemic hypertension, arrhythmia, congestive heart failure, valvular heart disease, vascular disease, congenital heart disease, and cardiomyopathy.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
