Fotios Barkas, Georgia Anastasiou, George Liamis, Haralampos Milionis
{"title":"A step-by-step guide for the diagnosis and management of hyponatraemia in patients with stroke.","authors":"Fotios Barkas, Georgia Anastasiou, George Liamis, Haralampos Milionis","doi":"10.1177/20420188231163806","DOIUrl":null,"url":null,"abstract":"<p><p>Hyponatraemia is common in patients with stroke and associated with adverse outcomes and increased mortality risk. The present review presents the underlying causes and provides a thorough algorithm for the diagnosis and management of hyponatraemia in stroke patients. Concomitant diseases and therapies, such as diabetes, chronic kidney disease and heart failure, along with diuretics, antidepressants and proton pump inhibitors are the most common causes of hyponatraemia in community. In the setting of acute stroke, the emergence of hyponatraemia might be attributed to the administration of hypotonic solutions and drugs (ie. mannitol and antiepileptics), poor solute intake, infections, as well as stroke-related conditions or complications, such as the syndrome of inappropriate secretion of antidiuretic hormone, cerebral salt wasting syndrome and secondary adrenal insufficiency. Diagnostically, the initial step is to differentiate hypotonic from non-hypotonic hyponatraemia, usually caused by hyperglycaemia or recent mannitol administration in patients with stroke. Determining urine osmolality, urine sodium level and volume status are the following steps in the differentiation of hypotonic hyponatraemia. Of note, specific parameters, such as fractional uric acid and urea excretion, along with plasma copeptin concentration, may further improve the diagnostic yield. Therapeutic options are based on the duration and symptoms of hyponatremia. In the case of acute or symptomatic hyponatraemia, hypertonic saline administration is recommended. Hypovolaemic chronic hyponatremia is treated with isotonic solution administration. Although fluid restriction remains the first-line treatment for the rest forms of chronic hyponatraemia, therapies increasing renal free water excretion may be necessary. Loop diuretics and urea serve this purpose in patients with stroke, whereas sodium-glucose transport protein-2 inhibitors appear to be a promising therapy. Nevertheless, it is yet unclear whether the appropriate restoration of sodium level improves outcomes in such patients. Randomized trials designed to compare therapeutic strategies in managing hyponatraemia in patients with stroke are required.</p>","PeriodicalId":22998,"journal":{"name":"Therapeutic Advances in Endocrinology and Metabolism","volume":"14 ","pages":"20420188231163806"},"PeriodicalIF":4.6000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a7/78/10.1177_20420188231163806.PMC10074625.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Endocrinology and Metabolism","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/20420188231163806","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 2
Abstract
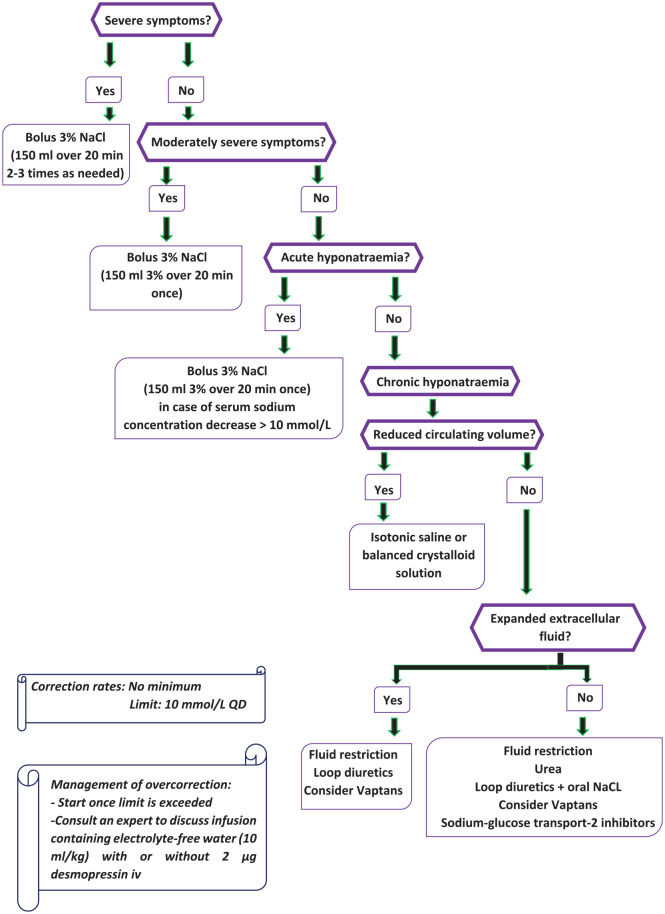
Hyponatraemia is common in patients with stroke and associated with adverse outcomes and increased mortality risk. The present review presents the underlying causes and provides a thorough algorithm for the diagnosis and management of hyponatraemia in stroke patients. Concomitant diseases and therapies, such as diabetes, chronic kidney disease and heart failure, along with diuretics, antidepressants and proton pump inhibitors are the most common causes of hyponatraemia in community. In the setting of acute stroke, the emergence of hyponatraemia might be attributed to the administration of hypotonic solutions and drugs (ie. mannitol and antiepileptics), poor solute intake, infections, as well as stroke-related conditions or complications, such as the syndrome of inappropriate secretion of antidiuretic hormone, cerebral salt wasting syndrome and secondary adrenal insufficiency. Diagnostically, the initial step is to differentiate hypotonic from non-hypotonic hyponatraemia, usually caused by hyperglycaemia or recent mannitol administration in patients with stroke. Determining urine osmolality, urine sodium level and volume status are the following steps in the differentiation of hypotonic hyponatraemia. Of note, specific parameters, such as fractional uric acid and urea excretion, along with plasma copeptin concentration, may further improve the diagnostic yield. Therapeutic options are based on the duration and symptoms of hyponatremia. In the case of acute or symptomatic hyponatraemia, hypertonic saline administration is recommended. Hypovolaemic chronic hyponatremia is treated with isotonic solution administration. Although fluid restriction remains the first-line treatment for the rest forms of chronic hyponatraemia, therapies increasing renal free water excretion may be necessary. Loop diuretics and urea serve this purpose in patients with stroke, whereas sodium-glucose transport protein-2 inhibitors appear to be a promising therapy. Nevertheless, it is yet unclear whether the appropriate restoration of sodium level improves outcomes in such patients. Randomized trials designed to compare therapeutic strategies in managing hyponatraemia in patients with stroke are required.
期刊介绍:
Therapeutic Advances in Endocrinology and Metabolism delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of endocrinology and metabolism.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
