Syed Mohammad Asim Hussain, Suzanne Cole, Iram Hussain
{"title":"Colorectal cancer metastases in thyroid: case report and literature review.","authors":"Syed Mohammad Asim Hussain, Suzanne Cole, Iram Hussain","doi":"10.1186/s13044-023-00150-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The thyroid gland is an uncommon site for metastatic deposits from non-thyroid malignancies, occurring in only 1.4 - 3% of surgical specimens where malignancy is suspected. It is even rarer for the source of thyroid metastases to be of colorectal origin. In most cases reported, colorectal metastases in the thyroid occurs many years later after the primary colorectal cancer has been diagnosed and treated. In this unique case, a primary sigmoid carcinoma metastasised to the thyroid gland and presented synchronously as a thyroid nodule.</p><p><strong>Case presentation: </strong>We describe a case of a 64-year-old Caucasian woman who presented with clinical features of metastatic cancer of unknown origin. Her medical history included underlying hyperthyroidism. She had a large pelvic mass adjacent to the sigmoid colon, a left lower lobe lung mass and a suspicious nodule in the left thyroid lobe. A fine-needle aspiration biopsy of the thyroid nodule was performed, which remarkably showed malignant cells originating from primary colorectal cancer on immunohistochemical staining. The patient was managed with palliative chemotherapy given the poor prognosis due to disseminated colorectal malignancy.</p><p><strong>Conclusions: </strong>Colorectal adenocarcinoma metastases can rarely present as a metastatic thyroid nodule. Fine-needle aspiration should be performed in suspicious thyroid nodules and may be the least invasive way of identifying a metastatic colorectal or other non-thyroidal malignancy in patients presenting with an unknown primary. The pathologist should be vigilant to this possibility and specific immunohistochemical markers should be used to ensure accurate diagnosis. In thyroid metastases, the prognosis is ultimately determined by the primary tumour but thyroidectomy still has a role in alleviating compressive symptoms and can potentially improve survival in selected cases.</p>","PeriodicalId":39048,"journal":{"name":"Thyroid Research","volume":"16 1","pages":"8"},"PeriodicalIF":1.8000,"publicationDate":"2023-04-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10084646/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thyroid Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13044-023-00150-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 1
Abstract
Background: The thyroid gland is an uncommon site for metastatic deposits from non-thyroid malignancies, occurring in only 1.4 - 3% of surgical specimens where malignancy is suspected. It is even rarer for the source of thyroid metastases to be of colorectal origin. In most cases reported, colorectal metastases in the thyroid occurs many years later after the primary colorectal cancer has been diagnosed and treated. In this unique case, a primary sigmoid carcinoma metastasised to the thyroid gland and presented synchronously as a thyroid nodule.
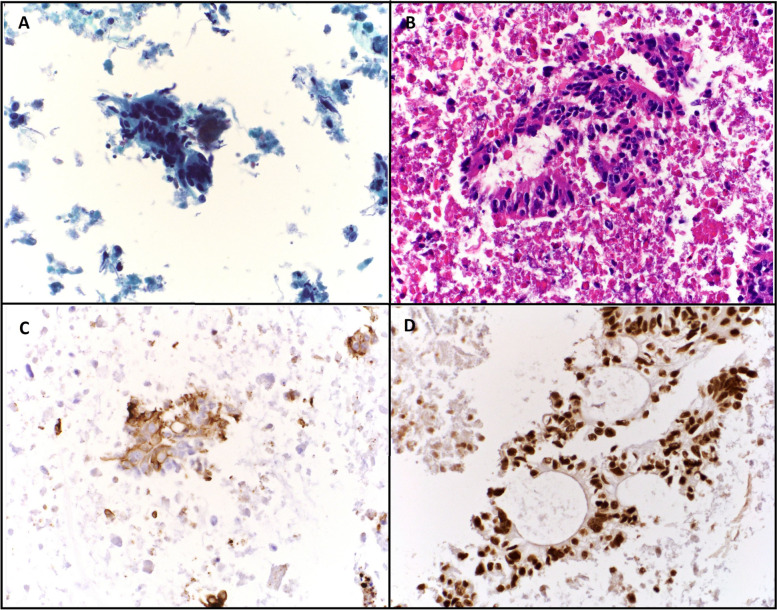
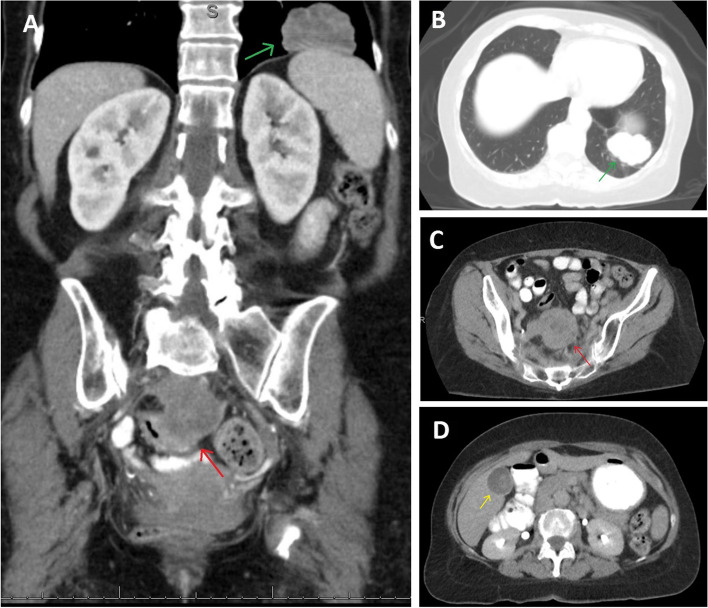
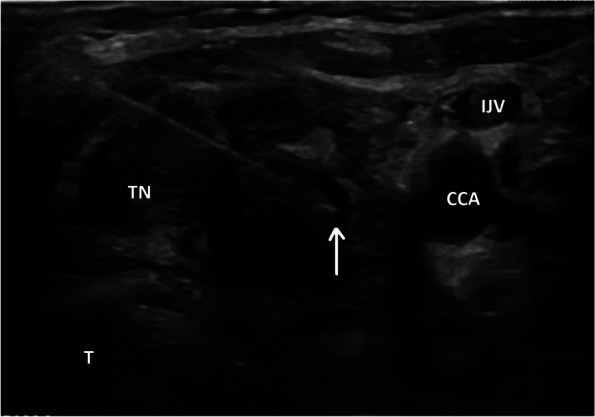
Case presentation: We describe a case of a 64-year-old Caucasian woman who presented with clinical features of metastatic cancer of unknown origin. Her medical history included underlying hyperthyroidism. She had a large pelvic mass adjacent to the sigmoid colon, a left lower lobe lung mass and a suspicious nodule in the left thyroid lobe. A fine-needle aspiration biopsy of the thyroid nodule was performed, which remarkably showed malignant cells originating from primary colorectal cancer on immunohistochemical staining. The patient was managed with palliative chemotherapy given the poor prognosis due to disseminated colorectal malignancy.
Conclusions: Colorectal adenocarcinoma metastases can rarely present as a metastatic thyroid nodule. Fine-needle aspiration should be performed in suspicious thyroid nodules and may be the least invasive way of identifying a metastatic colorectal or other non-thyroidal malignancy in patients presenting with an unknown primary. The pathologist should be vigilant to this possibility and specific immunohistochemical markers should be used to ensure accurate diagnosis. In thyroid metastases, the prognosis is ultimately determined by the primary tumour but thyroidectomy still has a role in alleviating compressive symptoms and can potentially improve survival in selected cases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
