Marianne Cecilie Johansen Nævra, Luis Romundstad, Anders Aasheim, Pål Gunnar Larsson
{"title":"Monitoring the Awake and Anesthetized Unconscious States Using Bispectral Index and Electroencephalographic Connectivity Measures.","authors":"Marianne Cecilie Johansen Nævra, Luis Romundstad, Anders Aasheim, Pål Gunnar Larsson","doi":"10.1177/15500594221131680","DOIUrl":null,"url":null,"abstract":"<p><p><i>Objective.</i> Our objective was to compare three electroencephalography (EEG)-based methods with anesthesiologist clinical judgment of the awake and anesthetized unconscious states. <i>Methods.</i> EEG recorded from 25 channels and from four channel bilateral Bispectral index (BIS) electrodes were collected from 20 patients undergoing surgery with general anesthesia. To measure connectivity we applied Directed Transfer Function (DTF) in eight channels of the EEG, and extracted data from BIS over the same time segments. Shannon's entropy was applied to assess the complexity of the EEG signal. Discriminant analysis was used to evaluate the data in relation to clinical judgment. <i>Results.</i> Assessing anesthetic state relative clinical judgment, the bilateral BIS gave the highest accuracy (ACC) (95.4%) and lowest false positive discovery rate (FDR) (0.5%) . Equivalent DTF gave 94.5% for ACC and 2.6% for FDR. Combining all methods gave ACC = 94.9% and FDR = 1%. Generally, entropy scored lower on ACC and higher on FDR than the other methods (ACC 90.87% and FDR 4.6%). BIS showed at least a one minute delay in 18 of the 20 patients. <i>Conclusions.</i> Our results show that BIS and DTF both have a high ACC and low FDR. Because of time delays in BIS values, we recommend combining the two methods.</p>","PeriodicalId":10682,"journal":{"name":"Clinical EEG and Neuroscience","volume":"54 3","pages":"273-280"},"PeriodicalIF":1.7000,"publicationDate":"2023-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4c/58/10.1177_15500594221131680.PMC10084521.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical EEG and Neuroscience","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/15500594221131680","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
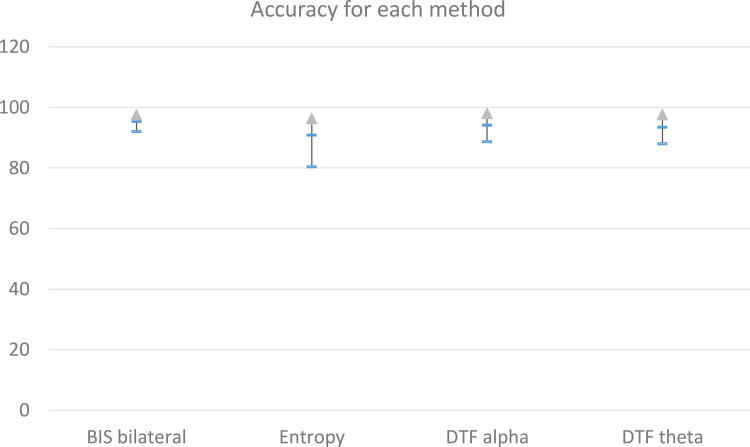
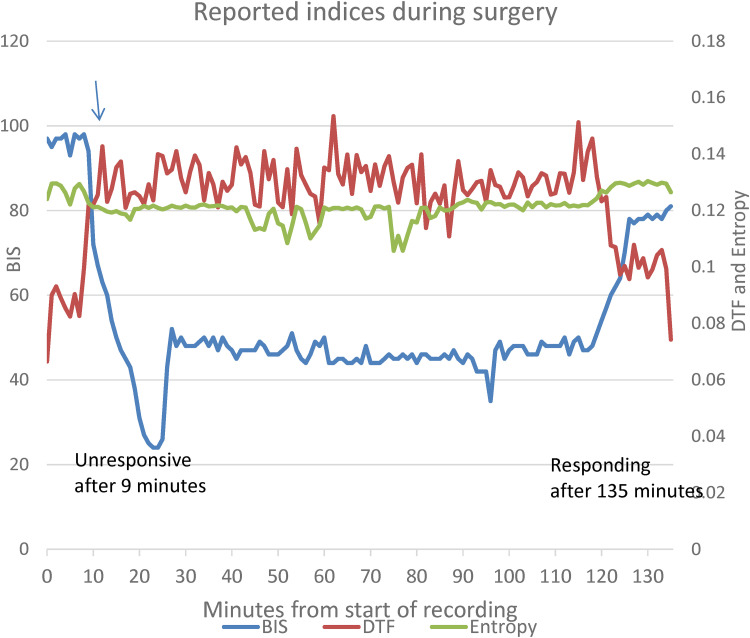
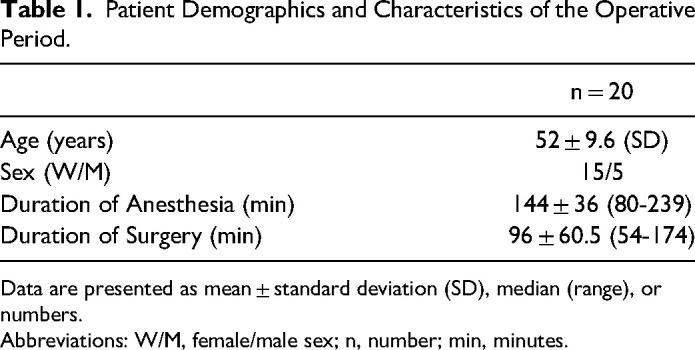
Objective. Our objective was to compare three electroencephalography (EEG)-based methods with anesthesiologist clinical judgment of the awake and anesthetized unconscious states. Methods. EEG recorded from 25 channels and from four channel bilateral Bispectral index (BIS) electrodes were collected from 20 patients undergoing surgery with general anesthesia. To measure connectivity we applied Directed Transfer Function (DTF) in eight channels of the EEG, and extracted data from BIS over the same time segments. Shannon's entropy was applied to assess the complexity of the EEG signal. Discriminant analysis was used to evaluate the data in relation to clinical judgment. Results. Assessing anesthetic state relative clinical judgment, the bilateral BIS gave the highest accuracy (ACC) (95.4%) and lowest false positive discovery rate (FDR) (0.5%) . Equivalent DTF gave 94.5% for ACC and 2.6% for FDR. Combining all methods gave ACC = 94.9% and FDR = 1%. Generally, entropy scored lower on ACC and higher on FDR than the other methods (ACC 90.87% and FDR 4.6%). BIS showed at least a one minute delay in 18 of the 20 patients. Conclusions. Our results show that BIS and DTF both have a high ACC and low FDR. Because of time delays in BIS values, we recommend combining the two methods.
期刊介绍:
Clinical EEG and Neuroscience conveys clinically relevant research and development in electroencephalography and neuroscience. Original articles on any aspect of clinical neurophysiology or related work in allied fields are invited for publication.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
