{"title":"Reconstruction of a Composite Defect of the Distal Index Finger Using a Chimeric Reverse Flow Second Dorsal Metacarpal Artery Flap: A Case Report.","authors":"Koichi Yano, Yasunori Kaneshiro, Megumi Ishiko, Seungho Hyun, Hideki Sakanaka","doi":"10.1055/s-0041-1731938","DOIUrl":null,"url":null,"abstract":"<p><p>The reconstruction for mild tissue loss at the distal part of a finger is challenging. We report about a 29-year-old man presenting with traumatic tissue loss at the distal interphalangeal (DIP) joint of the index finger, including skin, bone, and nerve. Reconstruction using two types of flaps was performed. The dorsal skin flap, nourished by the second dorsal metacarpal artery (SDMA) perforator, was elevated. The vascularized second metacarpal bone, nourished by the SDMA, was also elevated. Using the vascular connection between the DMA and the palmar digital artery (PDA), both flaps were raised to the distal part of the finger, and the pivot point was set at the dorsal proximal phalanx. After arthrodesis of the DIP joint with the vascularized second metacarpal bone, the digital nerve was repaired using the cutaneous nerve in the skin flap, and the skin defect was covered using the perforator flap. The postoperative course, including flap survival and bone union, was uneventful. A good indication for the reconstruction of the distal part of a finger with this technique is when the defect sizes of the skin and bone differ and the vascular connection between the SDMA and dorsal branch of PDA is not injured.</p>","PeriodicalId":45368,"journal":{"name":"Journal of Hand and Microsurgery","volume":"15 2","pages":"148-151"},"PeriodicalIF":0.5000,"publicationDate":"2021-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/33/fa/10-1055-s-0041-1731938.PMC10069996.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hand and Microsurgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0041-1731938","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/4/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
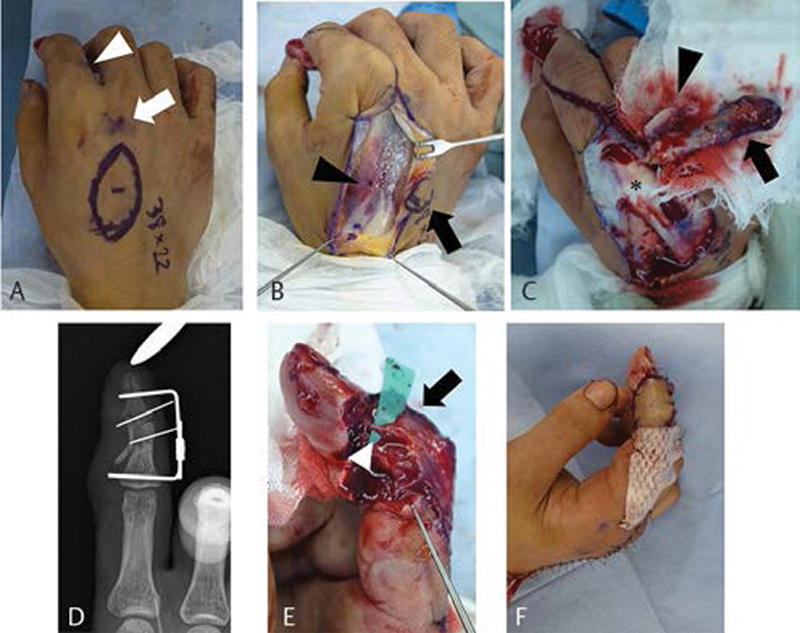
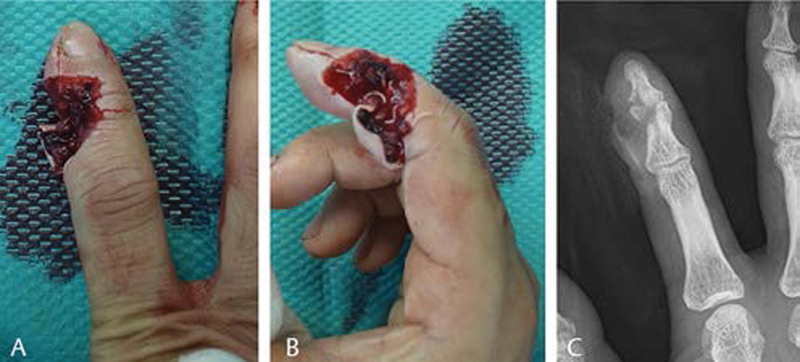
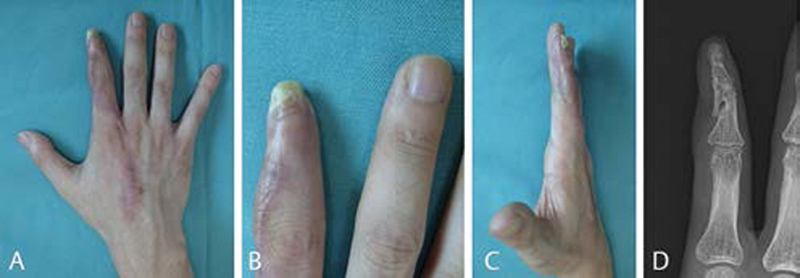
The reconstruction for mild tissue loss at the distal part of a finger is challenging. We report about a 29-year-old man presenting with traumatic tissue loss at the distal interphalangeal (DIP) joint of the index finger, including skin, bone, and nerve. Reconstruction using two types of flaps was performed. The dorsal skin flap, nourished by the second dorsal metacarpal artery (SDMA) perforator, was elevated. The vascularized second metacarpal bone, nourished by the SDMA, was also elevated. Using the vascular connection between the DMA and the palmar digital artery (PDA), both flaps were raised to the distal part of the finger, and the pivot point was set at the dorsal proximal phalanx. After arthrodesis of the DIP joint with the vascularized second metacarpal bone, the digital nerve was repaired using the cutaneous nerve in the skin flap, and the skin defect was covered using the perforator flap. The postoperative course, including flap survival and bone union, was uneventful. A good indication for the reconstruction of the distal part of a finger with this technique is when the defect sizes of the skin and bone differ and the vascular connection between the SDMA and dorsal branch of PDA is not injured.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
