Anas Almatrafi, Owen Thomas, Matthew Callister, Rhian Gabe, Rebecca J Beeken, Richard Neal
{"title":"The prevalence of comorbidity in the lung cancer screening population: A systematic review and meta-analysis.","authors":"Anas Almatrafi, Owen Thomas, Matthew Callister, Rhian Gabe, Rebecca J Beeken, Richard Neal","doi":"10.1177/09691413221117685","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Comorbidity is associated with adverse outcomes for all lung cancer patients, but its burden is less understood in the context of screening. This review synthesises the prevalence of comorbidities among lung cancer screening (LCS) candidates and summarises the clinical recommendations for screening comorbid individuals.</p><p><strong>Methods: </strong>We searched MEDLINE, EMBASE, EBM Reviews, and CINAHL databases from January 1990 to February 2021. We included LCS studies that reported a prevalence of comorbidity, as a prevalence of a particular condition, or as a summary score. We also summarised LCS clinical guidelines that addressed comorbidity or frailty for LCS as a secondary objective for this review. Meta-analysis was used with inverse-variance weights obtained from a random-effects model to estimate the prevalence of selected comorbidities.</p><p><strong>Results: </strong>We included 69 studies in the review; seven reported comorbidity summary scores, two reported performance status, 48 reported individual comorbidities, and 12 were clinical guideline papers. The meta-analysis of individual comorbidities resulted in an estimated prevalence of 35.2% for hypertension, 23.5% for history of chronic obstructive pulmonary disease (COPD) (10.7% for severe COPD), 16.6% for ischaemic heart disease (IHD), 13.1% for peripheral vascular disease (PVD), 12.9% for asthma, 12.5% for diabetes, 4.5% for bronchiectasis, 2.2% for stroke, and 0.5% for pulmonary fibrosis.</p><p><strong>Conclusions: </strong>Comorbidities were highly prevalent in LCS populations and likely to be more prevalent than in other cancer screening programmes. Further research on the burden of comorbid disease and its impact on screening uptake and outcomes is needed. Identifying individuals with frailty and comorbidities who might not benefit from screening should become a priority in LCS research.</p>","PeriodicalId":51089,"journal":{"name":"Journal of Medical Screening","volume":"30 1","pages":"3-13"},"PeriodicalIF":2.3000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/30/e3/10.1177_09691413221117685.PMC9925896.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medical Screening","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/09691413221117685","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/8/9 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Comorbidity is associated with adverse outcomes for all lung cancer patients, but its burden is less understood in the context of screening. This review synthesises the prevalence of comorbidities among lung cancer screening (LCS) candidates and summarises the clinical recommendations for screening comorbid individuals.
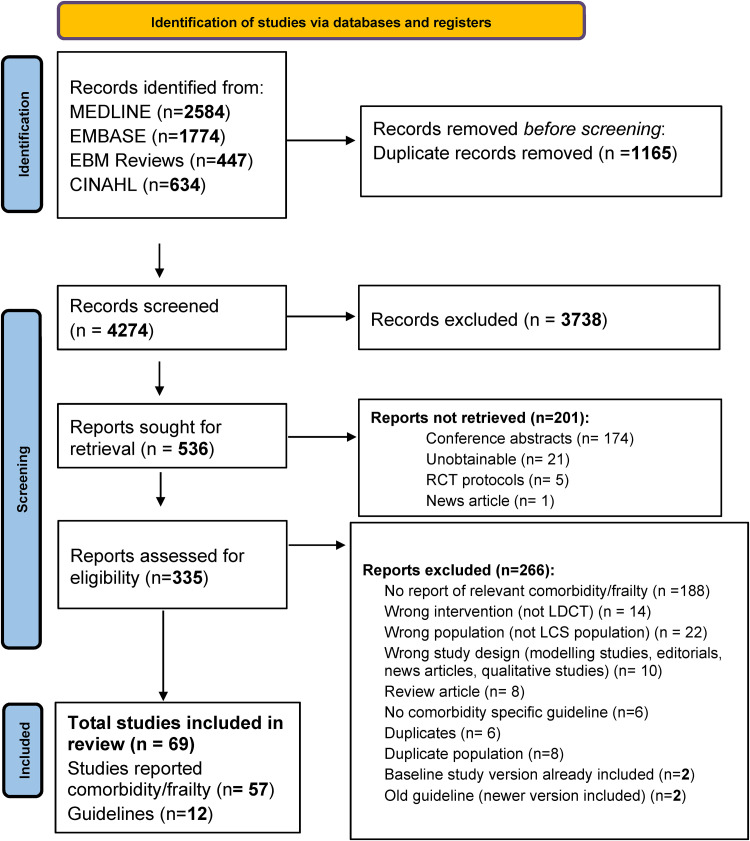
Methods: We searched MEDLINE, EMBASE, EBM Reviews, and CINAHL databases from January 1990 to February 2021. We included LCS studies that reported a prevalence of comorbidity, as a prevalence of a particular condition, or as a summary score. We also summarised LCS clinical guidelines that addressed comorbidity or frailty for LCS as a secondary objective for this review. Meta-analysis was used with inverse-variance weights obtained from a random-effects model to estimate the prevalence of selected comorbidities.
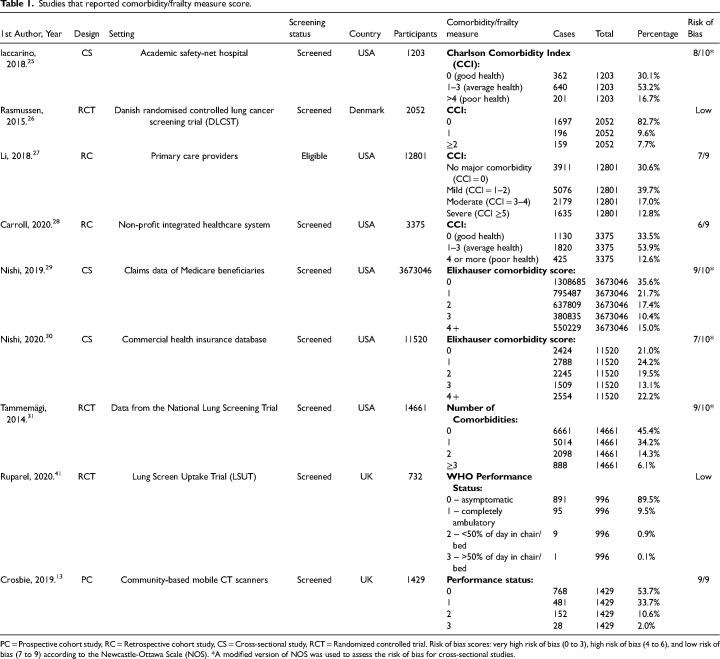
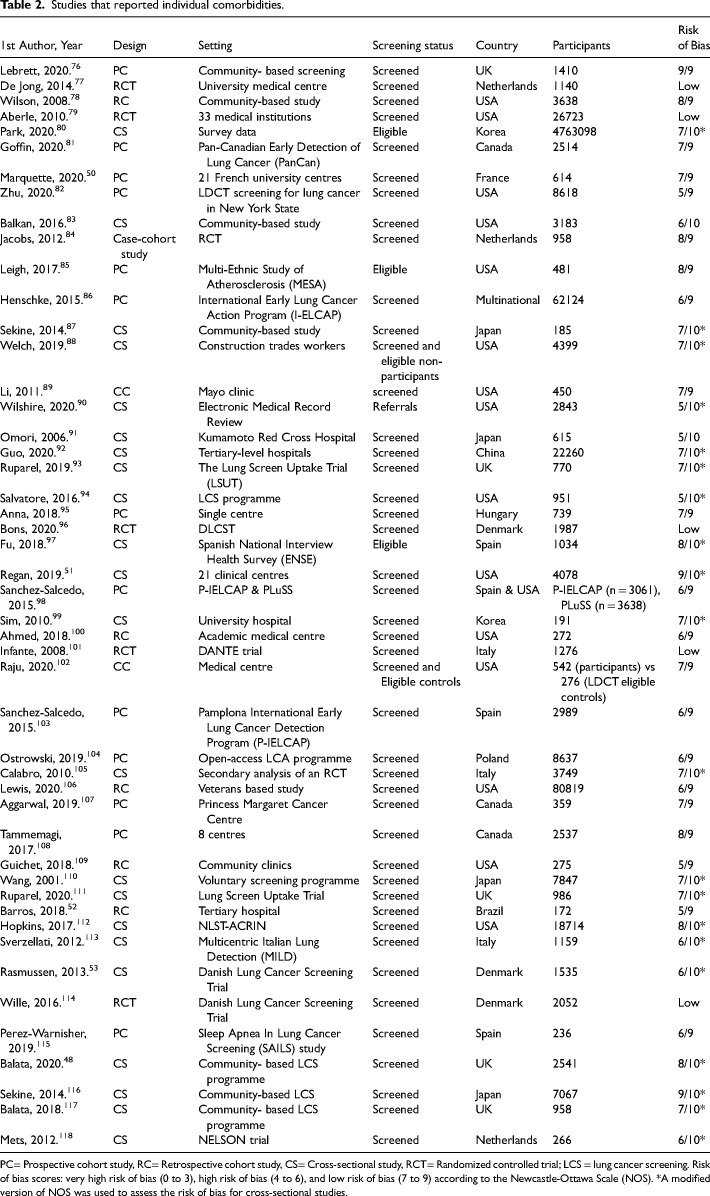
Results: We included 69 studies in the review; seven reported comorbidity summary scores, two reported performance status, 48 reported individual comorbidities, and 12 were clinical guideline papers. The meta-analysis of individual comorbidities resulted in an estimated prevalence of 35.2% for hypertension, 23.5% for history of chronic obstructive pulmonary disease (COPD) (10.7% for severe COPD), 16.6% for ischaemic heart disease (IHD), 13.1% for peripheral vascular disease (PVD), 12.9% for asthma, 12.5% for diabetes, 4.5% for bronchiectasis, 2.2% for stroke, and 0.5% for pulmonary fibrosis.
Conclusions: Comorbidities were highly prevalent in LCS populations and likely to be more prevalent than in other cancer screening programmes. Further research on the burden of comorbid disease and its impact on screening uptake and outcomes is needed. Identifying individuals with frailty and comorbidities who might not benefit from screening should become a priority in LCS research.
期刊介绍:
Journal of Medical Screening, a fully peer reviewed journal, is concerned with all aspects of medical screening, particularly the publication of research that advances screening theory and practice. The journal aims to increase awareness of the principles of screening (quantitative and statistical aspects), screening techniques and procedures and methodologies from all specialties. An essential subscription for physicians, clinicians and academics with an interest in screening, epidemiology and public health.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
