{"title":"Risk Factors for Postoperative Contralateral Hemorrhage in Patients With Traumatic Brain Injury who Underwent Surgical Treatment: A Multicenter Study.","authors":"In-Ho Jung, Jung-Ho Yun, Sang Koo Lee","doi":"10.13004/kjnt.2023.19.e3","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Patients with a contralateral intracranial hemorrhage after decompressive craniectomy have a worse prognosis than those whose recovery is uneventful. Therefore, the objective of this study was to identify risk factors for postoperative contralateral hemorrhage (PCH) in patients who underwent unilateral craniectomy or craniotomy due to a traumatic brain injury (TBI).</p><p><strong>Methods: </strong>Data were obtained from the Korean Neuro-Trauma Data Bank System and retrospectively reviewed. Patients who had a unilateral craniectomy or craniotomy for acute TBI were included in this study. Clinical outcomes of a PCH group and an uneventful group were compared and the risk factors for PCH were identified using regression analysis.</p><p><strong>Results: </strong>A total of 326 patients were included in this study. PCH was observed in 25 (7.7%) patients. The Glasgow coma scale (GCS) and Glasgow outcome scale extended (GOSE) scores at discharge were significantly lower in the PCH group than those in the uneventful group (GCS: 3.6 vs. 6.2, <i>p</i>=0.043; GOSE: 2.1 vs. 3.2, <i>p</i>=0.032). In the multivariable regression analysis, when the time from injury to surgery was shorter than 150 minutes, the risk of PCH was increased by 4.481 times (<i>p</i>=0.005). When the intraoperative transfusion volume was more than 1.5 L, the risk of PCH was increased by 4.843 times (<i>p</i>=0.003).</p><p><strong>Conclusion: </strong>The risk of PCH is increased when the time from injury to surgery is shorter than 150 minutes and when the intraoperative transfusion volume is greater than 1.5 L. Neurosurgeons must predict and be prepared for the development of PCH in high-risk patients.</p>","PeriodicalId":36879,"journal":{"name":"Korean Journal of Neurotrauma","volume":"19 1","pages":"42-52"},"PeriodicalIF":0.0000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ba/3b/kjn-19-42.PMC10083440.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Neurotrauma","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.13004/kjnt.2023.19.e3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Patients with a contralateral intracranial hemorrhage after decompressive craniectomy have a worse prognosis than those whose recovery is uneventful. Therefore, the objective of this study was to identify risk factors for postoperative contralateral hemorrhage (PCH) in patients who underwent unilateral craniectomy or craniotomy due to a traumatic brain injury (TBI).
Methods: Data were obtained from the Korean Neuro-Trauma Data Bank System and retrospectively reviewed. Patients who had a unilateral craniectomy or craniotomy for acute TBI were included in this study. Clinical outcomes of a PCH group and an uneventful group were compared and the risk factors for PCH were identified using regression analysis.
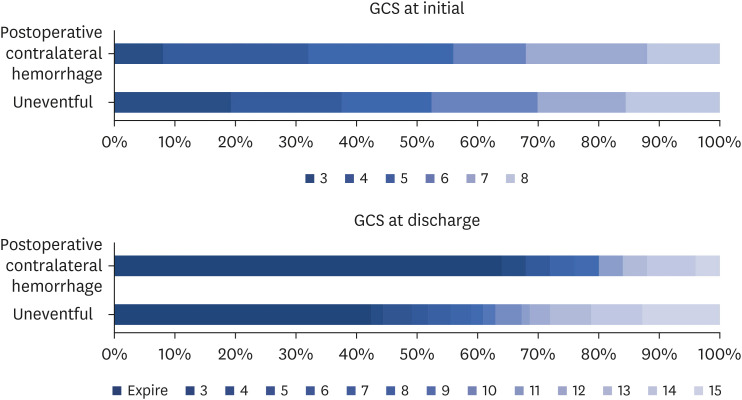
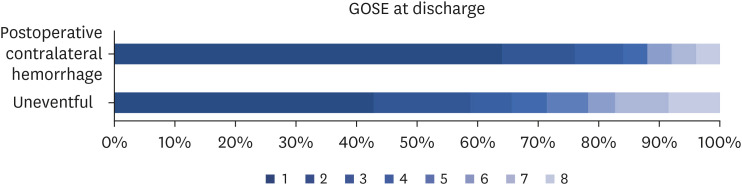
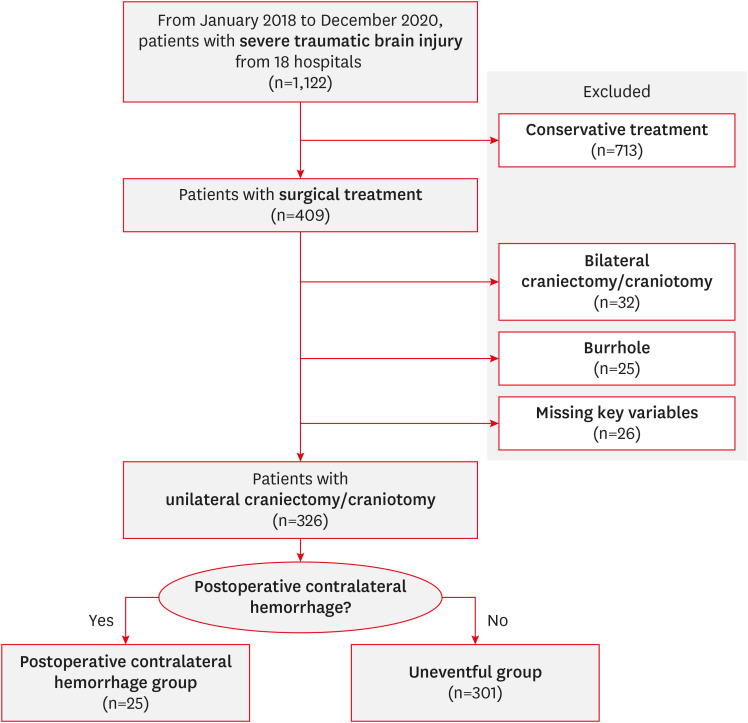
Results: A total of 326 patients were included in this study. PCH was observed in 25 (7.7%) patients. The Glasgow coma scale (GCS) and Glasgow outcome scale extended (GOSE) scores at discharge were significantly lower in the PCH group than those in the uneventful group (GCS: 3.6 vs. 6.2, p=0.043; GOSE: 2.1 vs. 3.2, p=0.032). In the multivariable regression analysis, when the time from injury to surgery was shorter than 150 minutes, the risk of PCH was increased by 4.481 times (p=0.005). When the intraoperative transfusion volume was more than 1.5 L, the risk of PCH was increased by 4.843 times (p=0.003).
Conclusion: The risk of PCH is increased when the time from injury to surgery is shorter than 150 minutes and when the intraoperative transfusion volume is greater than 1.5 L. Neurosurgeons must predict and be prepared for the development of PCH in high-risk patients.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
