{"title":"Challenges of Management of Ruptured Second Trimester Ovarian Pregnancy in Low-and Middle-Income Settings: A Case Report.","authors":"George Uchenna Eleje, Gerald Okanandu Udigwe, Tobechi Kingsley Njoku, Chukwuemeka Chukwubuikem Okoro, Chukwudubem Chinagorom Onyejiaka, Eric Chukwudi Ihekwoaba, Chinedu Onwuka Ndukwe, Onyedika Promise Anaedu, Michael Emeka Chiemeka, Chigozie Geoffrey Okafor, Onyeka Chukwudalu Ekwebene, Confidence Chinaza Offor, Odili Aloysius Okoye, Perpetua Chinedu Okolie, Divinefavour Echezona Malachy, Chimdindu Ifunanya Maduagwu, Jane-Rita Ifeoma Mmuotoo, Ekeuda Uchenna Nwankwo, Chimezuru Ogechi Duru, Emeka Philip Igbodike, Nnaedozie Paul Obiegbu, Joy Chisom Agbo, Nwabueze Chidozie Okeke, Ogonna Onyeka Ezenwafor, Henry Chinedu Nneji, Ogechi Odinakachukwu Dimgba, James Egwuatu Okonkwo","doi":"10.1177/11795476231153285","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Ovarian ectopic pregnancy is a rare form of non-tubal ectopic pregnancy. It can rupture before the end of the first trimester, causing hemoperitoneum, and present with signs and symptoms similar to other commoner abdominal emergencies or the pregnancy can continue intraperitoneally. Therefore, they are not often diagnosed preoperatively. Ultrasound can assist in diagnosis of ovarian ectopic pregnancy but the findings could be ambiguous or inconclusive. We present a case of ruptured ovarian ectopic pregnancy at the second trimester causing massive hemoperitoneum that was suspected as an intrabdominal malignancy co-existing with intrabdominal pregnancy.</p><p><strong>Case presentation: </strong>She was a 34 year-old Nigerian unbooked G4P3+0, (3 alive), who presented to the labor ward on 21st January, 2021 with a complaint of a 6-week history of abdominal pain and swelling. Pain was insidious in onset, generalized, non-colicky, non-radiating, constant, no known aggravating or relieving factor, but it was of moderate intensity. She had amenorrhea with a positive serum pregnancy test without prior early ultrasound. At presentation, initial abdominopelvic ultrasound revealed intra-uterine viable pregnancy but repeat ultrasound done showed a left adnexal ectopic gestation and an echo-rich intraperitoneal fluid collection. Laparotomy was done and ovarian pregnancy was accurately diagnosed intra-operatively. Tissue samples from the ovary confirmed normal products of conception, namely chorionic villi, trophoblastic cells and ovarian stroma at histology.</p><p><strong>Conclusion: </strong>Despite advances in imaging techniques, the diagnosis of ovarian ectopic gestation is still very difficult. When premenopausal women present with amenorrhea, generalized non-colicky abdominal pain and swelling in combination with ambiguous findings of pregnancy on ultrasound in the absence of trauma, differential diagnoses should include ruptured ovarian pregnancy. Obstetricians should maintain a high index of suspicion to forestall delayed diagnosis and the potential maternal morbidity and mortality. However, the need for high-index of suspicion should be for any ectopic, not just ovarian pregnancy.</p>","PeriodicalId":10357,"journal":{"name":"Clinical Medicine Insights. Case Reports","volume":"16 ","pages":"11795476231153285"},"PeriodicalIF":0.6000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2d/a0/10.1177_11795476231153285.PMC9926361.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795476231153285","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Ovarian ectopic pregnancy is a rare form of non-tubal ectopic pregnancy. It can rupture before the end of the first trimester, causing hemoperitoneum, and present with signs and symptoms similar to other commoner abdominal emergencies or the pregnancy can continue intraperitoneally. Therefore, they are not often diagnosed preoperatively. Ultrasound can assist in diagnosis of ovarian ectopic pregnancy but the findings could be ambiguous or inconclusive. We present a case of ruptured ovarian ectopic pregnancy at the second trimester causing massive hemoperitoneum that was suspected as an intrabdominal malignancy co-existing with intrabdominal pregnancy.
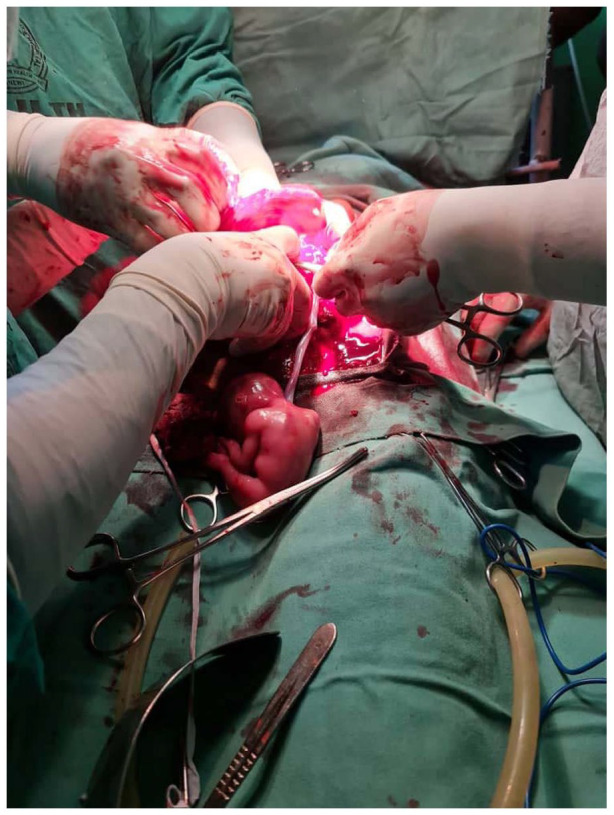
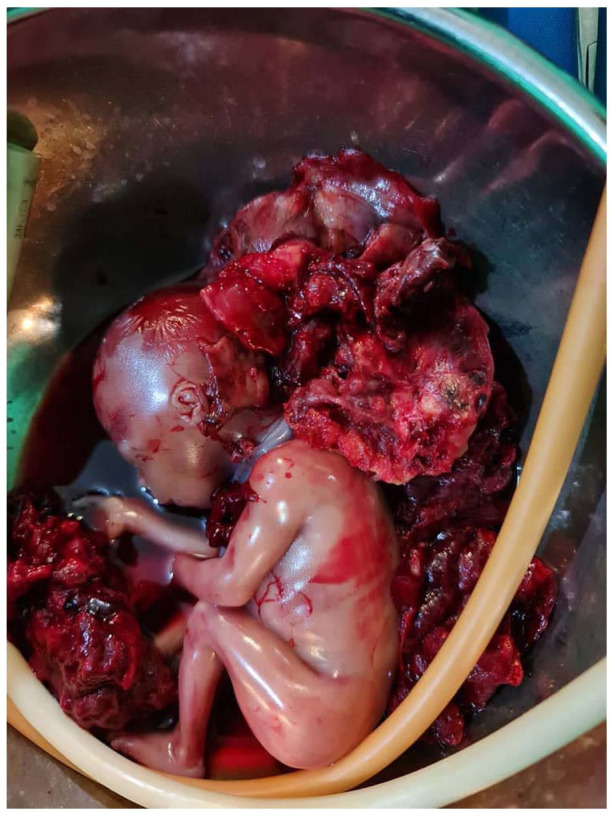
Case presentation: She was a 34 year-old Nigerian unbooked G4P3+0, (3 alive), who presented to the labor ward on 21st January, 2021 with a complaint of a 6-week history of abdominal pain and swelling. Pain was insidious in onset, generalized, non-colicky, non-radiating, constant, no known aggravating or relieving factor, but it was of moderate intensity. She had amenorrhea with a positive serum pregnancy test without prior early ultrasound. At presentation, initial abdominopelvic ultrasound revealed intra-uterine viable pregnancy but repeat ultrasound done showed a left adnexal ectopic gestation and an echo-rich intraperitoneal fluid collection. Laparotomy was done and ovarian pregnancy was accurately diagnosed intra-operatively. Tissue samples from the ovary confirmed normal products of conception, namely chorionic villi, trophoblastic cells and ovarian stroma at histology.
Conclusion: Despite advances in imaging techniques, the diagnosis of ovarian ectopic gestation is still very difficult. When premenopausal women present with amenorrhea, generalized non-colicky abdominal pain and swelling in combination with ambiguous findings of pregnancy on ultrasound in the absence of trauma, differential diagnoses should include ruptured ovarian pregnancy. Obstetricians should maintain a high index of suspicion to forestall delayed diagnosis and the potential maternal morbidity and mortality. However, the need for high-index of suspicion should be for any ectopic, not just ovarian pregnancy.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
