{"title":"Operative Timing and Feasibility of Mitral Valve Repair in Active Infective Endocarditis.","authors":"Tadashi Omoto, Atsushi Aoki, Kazuto Maruta, Tomoaki Masuda","doi":"10.5761/atcs.oa.22-00135","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>We studied the association between operative timing and the feasibility of mitral valve (MV) repair in active infective endocarditis (IE).</p><p><strong>Methods: </strong>Forty-nine active IE patients who underwent MV operation were classified according to operative timing: within 48 hours (Term I: n = 7), between 3 and 14 days (Term II: n = 22), and ≥15 days (Term III: n = 20). Patient profiles, operative outcomes, and feasibility of MV repair were evaluated. Complexity score and severity score were used to define the feasibility of MV repair depending on the extent of infected lesion and technical difficulties.</p><p><strong>Results: </strong>There were no differences in basic profile in the three groups. Rate of major complications was higher in Term I (86%) than II (41%, p = 0.031) and III (25%, p = 0.005). In-hospital mortality was also higher in Term I (43%) than II (9%, p = 0.039) and III (5%, p = 0.015). The three groups did not differ by feasibility of MV repair calculated by the two-score system or by frequency of MV repair (I: 57%, II: 59%, and III: 55%).</p><p><strong>Conclusions: </strong>Morbidity and mortality were high in urgent cases. Feasibility of MV repair is associated with the extent of infected lesion and technical difficulties, and not with operative timing.</p>","PeriodicalId":8037,"journal":{"name":"Annals of Thoracic and Cardiovascular Surgery","volume":"29 1","pages":"23-28"},"PeriodicalIF":1.3000,"publicationDate":"2023-02-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/77/4a/atcs-29-023.PMC9939675.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5761/atcs.oa.22-00135","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/11/3 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: We studied the association between operative timing and the feasibility of mitral valve (MV) repair in active infective endocarditis (IE).
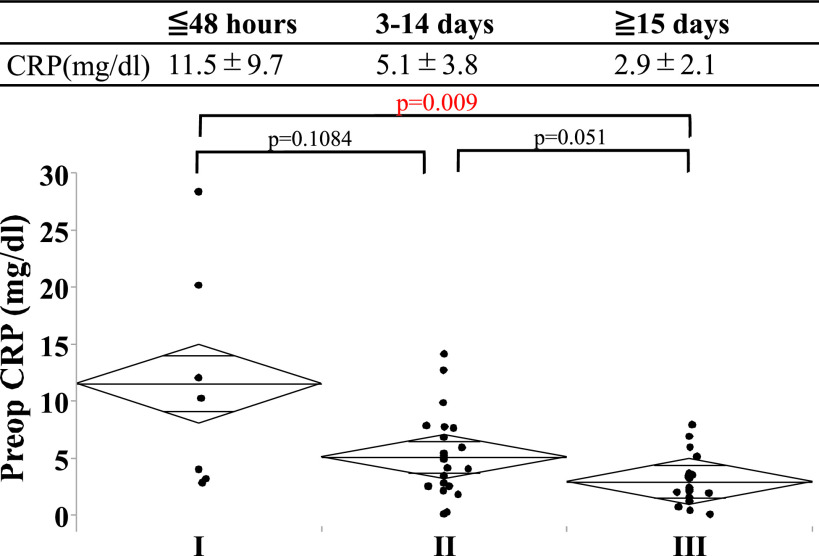
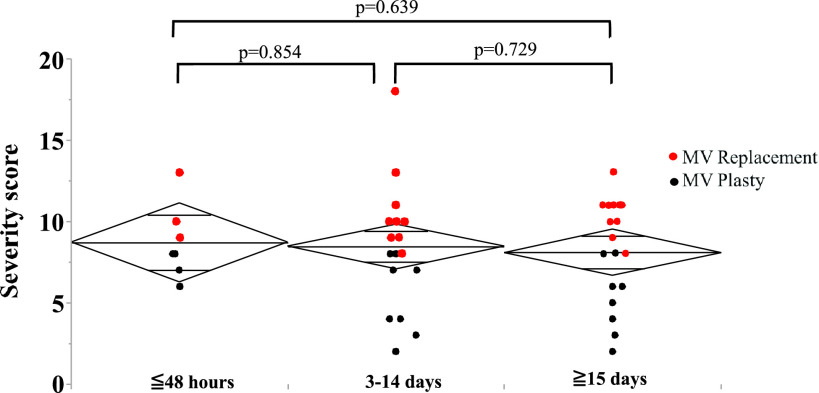
Methods: Forty-nine active IE patients who underwent MV operation were classified according to operative timing: within 48 hours (Term I: n = 7), between 3 and 14 days (Term II: n = 22), and ≥15 days (Term III: n = 20). Patient profiles, operative outcomes, and feasibility of MV repair were evaluated. Complexity score and severity score were used to define the feasibility of MV repair depending on the extent of infected lesion and technical difficulties.
Results: There were no differences in basic profile in the three groups. Rate of major complications was higher in Term I (86%) than II (41%, p = 0.031) and III (25%, p = 0.005). In-hospital mortality was also higher in Term I (43%) than II (9%, p = 0.039) and III (5%, p = 0.015). The three groups did not differ by feasibility of MV repair calculated by the two-score system or by frequency of MV repair (I: 57%, II: 59%, and III: 55%).
Conclusions: Morbidity and mortality were high in urgent cases. Feasibility of MV repair is associated with the extent of infected lesion and technical difficulties, and not with operative timing.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
