Jake Krige, Eduard Jonas, Chanel Robinson, Steve Beningfield, Urda Kotze, Marc Bernon, Sean Burmeister, Christo Kloppers
{"title":"Novel CABIN score outperforms other prognostic models in predicting in-hospital mortality after salvage transjugular intrahepatic portosystemic shunting.","authors":"Jake Krige, Eduard Jonas, Chanel Robinson, Steve Beningfield, Urda Kotze, Marc Bernon, Sean Burmeister, Christo Kloppers","doi":"10.4291/wjgp.v14.i2.34","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Transjugular intrahepatic portosystemic shunt (TIPS) is now established as the salvage procedure of choice in patients who have uncontrolled or severe recurrent variceal bleeding despite optimal medical and endoscopic treatment.</p><p><strong>Aim: </strong>To analysis compared the performance of eight risk scores to predict in-hospital mortality after salvage TIPS (sTIPS) placement in patients with uncontrolled variceal bleeding after failed medical treatment and endoscopic intervention.</p><p><strong>Methods: </strong>Baseline risk scores for the Acute Physiology and Chronic Health Evaluation (APACHE) II, Bonn TIPS early mortality (BOTEM), Child-Pugh, Emory, FIPS, model for end-stage liver disease (MELD), MELD-Na, and a novel 5 category CABIN score incorporating Creatinine, Albumin, Bilirubin, INR and Na, were calculated before sTIPS. Concordance (C) statistics for predictive accuracy of in-hospital mortality of the eight scores were compared using area under the receiver operating characteristic curve (AUROC) analysis.</p><p><strong>Results: </strong>Thirty-four patients (29 men, 5 women), median age 52 years (range 31-80) received sTIPS for uncontrolled (11) or refractory (23) bleeding between August 1991 and November 2020. Salvage TIPS controlled bleeding in 32 (94%) patients with recurrence in one. Ten (29%) patients died in hospital. All scoring systems had a significant association with in-hospital mortality (<i>P</i> < 0.05) on multivariate analysis. Based on in-hospital survival AUROC, the CABIN (0.967), APACHE II (0.948) and Emory (0.942) scores had the best capability predicting mortality compared to FIPS (0.892), BOTEM (0.877), MELD Na (0.865), Child-Pugh (0.802) and MELD (0.792).</p><p><strong>Conclusion: </strong>The novel CABIN score had the best prediction capability with statistical superiority over seven other risk scores. Despite sTIPS, hospital mortality remains high and can be predicted by CABIN category B or C or CABIN scores > 10. Survival was 100% in CABIN A patients while mortality was 75% for CABIN B, 87.5% for CABIN C, and 83% for CABIN scores > 10.</p>","PeriodicalId":23760,"journal":{"name":"World Journal of Gastrointestinal Pathophysiology","volume":"14 2","pages":"34-45"},"PeriodicalIF":0.0000,"publicationDate":"2023-03-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0d/92/WJGP-14-34.PMC10074947.pdf","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Pathophysiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4291/wjgp.v14.i2.34","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
Background: Transjugular intrahepatic portosystemic shunt (TIPS) is now established as the salvage procedure of choice in patients who have uncontrolled or severe recurrent variceal bleeding despite optimal medical and endoscopic treatment.
Aim: To analysis compared the performance of eight risk scores to predict in-hospital mortality after salvage TIPS (sTIPS) placement in patients with uncontrolled variceal bleeding after failed medical treatment and endoscopic intervention.
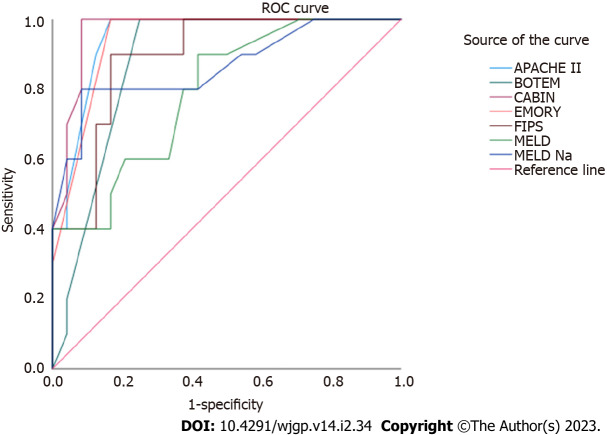
Methods: Baseline risk scores for the Acute Physiology and Chronic Health Evaluation (APACHE) II, Bonn TIPS early mortality (BOTEM), Child-Pugh, Emory, FIPS, model for end-stage liver disease (MELD), MELD-Na, and a novel 5 category CABIN score incorporating Creatinine, Albumin, Bilirubin, INR and Na, were calculated before sTIPS. Concordance (C) statistics for predictive accuracy of in-hospital mortality of the eight scores were compared using area under the receiver operating characteristic curve (AUROC) analysis.
Results: Thirty-four patients (29 men, 5 women), median age 52 years (range 31-80) received sTIPS for uncontrolled (11) or refractory (23) bleeding between August 1991 and November 2020. Salvage TIPS controlled bleeding in 32 (94%) patients with recurrence in one. Ten (29%) patients died in hospital. All scoring systems had a significant association with in-hospital mortality (P < 0.05) on multivariate analysis. Based on in-hospital survival AUROC, the CABIN (0.967), APACHE II (0.948) and Emory (0.942) scores had the best capability predicting mortality compared to FIPS (0.892), BOTEM (0.877), MELD Na (0.865), Child-Pugh (0.802) and MELD (0.792).
Conclusion: The novel CABIN score had the best prediction capability with statistical superiority over seven other risk scores. Despite sTIPS, hospital mortality remains high and can be predicted by CABIN category B or C or CABIN scores > 10. Survival was 100% in CABIN A patients while mortality was 75% for CABIN B, 87.5% for CABIN C, and 83% for CABIN scores > 10.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
