Laura Ann Rechner, Maja V Maraldo, Edward Ak Smith, Anni Y Lundgaard, Lisa L Hjalgrim, Ranald I MacKay, Adam H Aitkenhead, Marianne C Aznar
{"title":"Proton linear energy transfer and variable relative biological effectiveness for adolescent patients with Hodgkin lymphoma.","authors":"Laura Ann Rechner, Maja V Maraldo, Edward Ak Smith, Anni Y Lundgaard, Lisa L Hjalgrim, Ranald I MacKay, Adam H Aitkenhead, Marianne C Aznar","doi":"10.1259/bjro.20230012","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Proton therapy has a theoretical dosimetric advantage due to the Bragg peak, but the linear energy transfer (LET), and therefore the relative biological effectiveness (RBE), increase at the end of range. For patients with Hodgkin lymphoma, the distal edge of beam is often located within or close to the heart, where elevated RBE would be of potential concern. The purpose of this study was to investigate the impact of RBE and the choice of beam arrangement for adolescent patients with mediastinal Hodgkin lymphoma.</p><p><strong>Methods: </strong>For three previously treated adolescent patients, proton plans with 1-3 fields were created to a prescribed dose of 19.8 Gy (RBE) in 11 fractions (Varian Eclipse v13.7), assuming an RBE of 1.1. Plans were recalculated using Monte-Carlo (Geant4 v10.3.3/Gate v8.1) to calculate dose-averaged LET. Variable RBE-weighted dose was calculated using the McNamara model, assuming an α/β ratio of 2 Gy for organs-at-risk.</p><p><strong>Results: </strong>Although the LET decreased as the number of fields increased, the difference in RBE-weighted dose (Δdose) to organs-at-risk did not consistently decrease. Δdose values varied by patient and organ and were mostly of the order of 0-3 Gy (RBE), with a worst-case of 4.75 Gy (RBE) in near-maximum dose to the left atrium for one plan.</p><p><strong>Conclusions: </strong>RBE-weighted doses to organs-at-risk are sensitive to the choice of RBE model, which is of particular concern for the heart.</p><p><strong>Advances in knowledge: </strong>There is a need to remain cautious when evaluating proton plans for Hodgkin lymphoma, especially when near-maximum doses to organs-at-risk are considered.</p>","PeriodicalId":72419,"journal":{"name":"BJR open","volume":"5 1","pages":"20230012"},"PeriodicalIF":2.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10077416/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJR open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1259/bjro.20230012","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
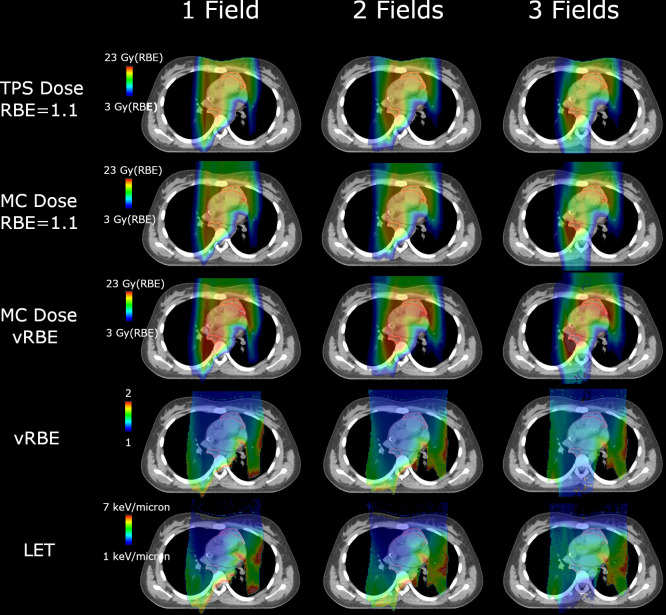
Objectives: Proton therapy has a theoretical dosimetric advantage due to the Bragg peak, but the linear energy transfer (LET), and therefore the relative biological effectiveness (RBE), increase at the end of range. For patients with Hodgkin lymphoma, the distal edge of beam is often located within or close to the heart, where elevated RBE would be of potential concern. The purpose of this study was to investigate the impact of RBE and the choice of beam arrangement for adolescent patients with mediastinal Hodgkin lymphoma.
Methods: For three previously treated adolescent patients, proton plans with 1-3 fields were created to a prescribed dose of 19.8 Gy (RBE) in 11 fractions (Varian Eclipse v13.7), assuming an RBE of 1.1. Plans were recalculated using Monte-Carlo (Geant4 v10.3.3/Gate v8.1) to calculate dose-averaged LET. Variable RBE-weighted dose was calculated using the McNamara model, assuming an α/β ratio of 2 Gy for organs-at-risk.
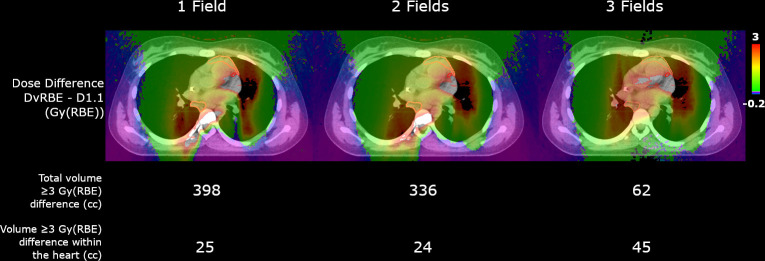
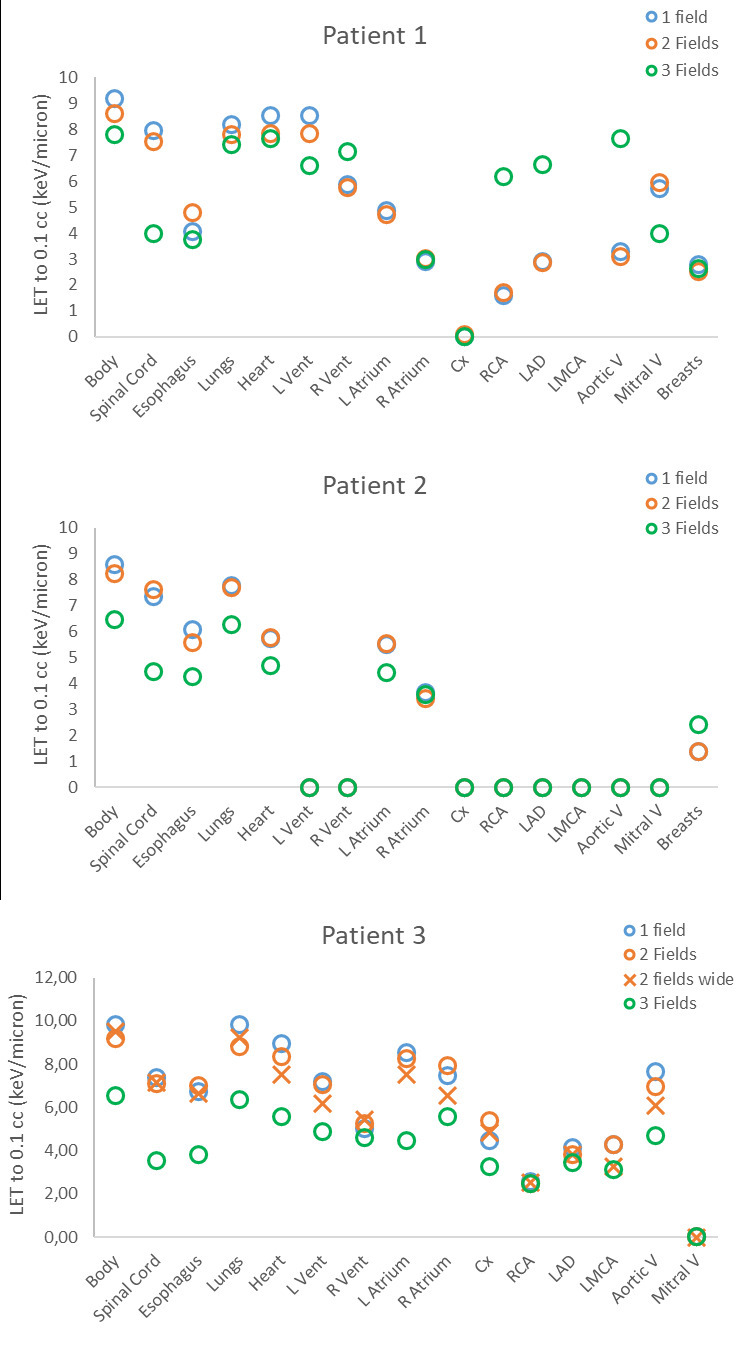
Results: Although the LET decreased as the number of fields increased, the difference in RBE-weighted dose (Δdose) to organs-at-risk did not consistently decrease. Δdose values varied by patient and organ and were mostly of the order of 0-3 Gy (RBE), with a worst-case of 4.75 Gy (RBE) in near-maximum dose to the left atrium for one plan.
Conclusions: RBE-weighted doses to organs-at-risk are sensitive to the choice of RBE model, which is of particular concern for the heart.
Advances in knowledge: There is a need to remain cautious when evaluating proton plans for Hodgkin lymphoma, especially when near-maximum doses to organs-at-risk are considered.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
