Outcomes after peripheral artery disease intervention among Medicare-Medicaid dual-eligible patients compared with the general medicare population in the Vascular Quality Initiative registry.
Andrea M Austin, Gouri Chakraborti, Jesse Columbo, Niveditta Ramkumar, Kayla Moore, Michelle Scheurich, Phil Goodney
{"title":"Outcomes after peripheral artery disease intervention among Medicare-Medicaid dual-eligible patients compared with the general medicare population in the Vascular Quality Initiative registry.","authors":"Andrea M Austin, Gouri Chakraborti, Jesse Columbo, Niveditta Ramkumar, Kayla Moore, Michelle Scheurich, Phil Goodney","doi":"10.1136/bmjsit-2019-000018","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To determine whether patients from the Vascular Quality Initiative (VQI) registry who are Medicare-Medicaid dual-eligible have outcomes after surgical intervention with medical devices such as stents for peripheral artery disease comparable to the outcomes of those eligible for Medicare alone.</p><p><strong>Methods: </strong>The study cohort included fee-for-service Medicare beneficiaries from 2010 to 2015 who underwent peripheral vascular intervention as determined by the VQI. We performed propensity matching between the dual-eligible and non-dual-eligible cohorts. Postintervention use, including imaging, amputation and death, was determined using Medicare claims data.</p><p><strong>Results: </strong>Rates of major amputation were higher among dual-eligible patients (13.0% vs 10.5%, p<0.001), while time to amputation by disease severity was similar (p=0.443). For patients with more advanced disease (critical limb ischaemia (CLI) vs claudication), dual-eligible patients have significantly faster times to any amputation and death (p<0.001). For of postoperative imaging, 48.4% of dual-eligible patients receive at least one postoperative image, while the percentage for non-dual-eligible patients is 47.2% (p=0.187).</p><p><strong>Conclusions: </strong>Patients with mild forms of peripheral artery disease (PAD), such as claudication, demonstrated similar outcomes regardless of dual-eligibility status. However, those with severe PAD, such as CLI, who were also dual-eligible had both inferior overall survival and amputation-free survival. Minimal differences were observed in process-driven aspects of care between dual-eligible and non-dual-eligible patients, including postoperative imaging. These findings indicate that despite receiving similar care, dual-eligible patients with severe PAD have inferior long-term outcomes, suggesting the Medicaid safety net is not timely enough to benefit from long-term outcomes for these patients.</p>","PeriodicalId":33349,"journal":{"name":"BMJ Surgery Interventions Health Technologies","volume":"1 1","pages":"e000018"},"PeriodicalIF":1.6000,"publicationDate":"2019-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8e/16/bmjsit-2019-000018.PMC7164790.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Surgery Interventions Health Technologies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjsit-2019-000018","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To determine whether patients from the Vascular Quality Initiative (VQI) registry who are Medicare-Medicaid dual-eligible have outcomes after surgical intervention with medical devices such as stents for peripheral artery disease comparable to the outcomes of those eligible for Medicare alone.
Methods: The study cohort included fee-for-service Medicare beneficiaries from 2010 to 2015 who underwent peripheral vascular intervention as determined by the VQI. We performed propensity matching between the dual-eligible and non-dual-eligible cohorts. Postintervention use, including imaging, amputation and death, was determined using Medicare claims data.
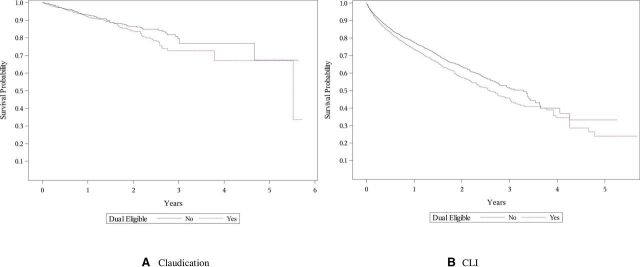
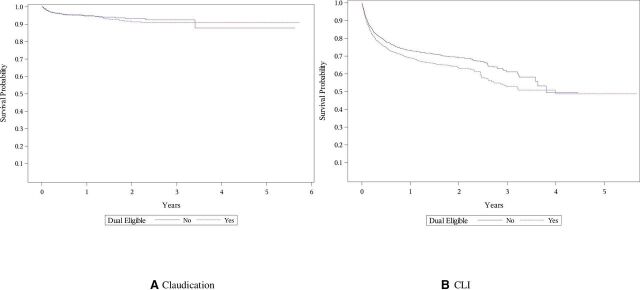
Results: Rates of major amputation were higher among dual-eligible patients (13.0% vs 10.5%, p<0.001), while time to amputation by disease severity was similar (p=0.443). For patients with more advanced disease (critical limb ischaemia (CLI) vs claudication), dual-eligible patients have significantly faster times to any amputation and death (p<0.001). For of postoperative imaging, 48.4% of dual-eligible patients receive at least one postoperative image, while the percentage for non-dual-eligible patients is 47.2% (p=0.187).
Conclusions: Patients with mild forms of peripheral artery disease (PAD), such as claudication, demonstrated similar outcomes regardless of dual-eligibility status. However, those with severe PAD, such as CLI, who were also dual-eligible had both inferior overall survival and amputation-free survival. Minimal differences were observed in process-driven aspects of care between dual-eligible and non-dual-eligible patients, including postoperative imaging. These findings indicate that despite receiving similar care, dual-eligible patients with severe PAD have inferior long-term outcomes, suggesting the Medicaid safety net is not timely enough to benefit from long-term outcomes for these patients.
目的:确定在血管质量倡议(VQI)登记的符合医疗-医疗补助双重资格的患者,在使用医疗器械(如外周动脉疾病支架)进行手术干预后的结果是否与仅符合医疗保险资格的患者的结果相当。方法:研究队列包括2010年至2015年接受外周血管干预(由VQI确定)的按服务收费的医疗保险受益人。我们在双重符合条件和非双重符合条件的队列之间进行倾向匹配。干预后的使用,包括成像、截肢和死亡,使用医疗保险索赔数据确定。结果:双重资格患者的主要截肢率更高(13.0% vs 10.5%)。结论:轻度外周动脉疾病(PAD)患者,如跛行,无论双重资格状态如何,均表现出相似的结果。然而,重度PAD患者(如CLI)的总生存期和无截肢生存期均较差。在双重合格和非双重合格患者的过程驱动方面,包括术后成像,观察到最小的差异。这些发现表明,尽管接受了类似的治疗,但双重资格的严重PAD患者的长期预后较差,这表明医疗补助安全网不够及时,无法从这些患者的长期预后中获益。



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
