L Russell, R Howard, M Street, C E Johnson, D Berry, E Flemming-Judge, S Brean, L William, J Considine
{"title":"Cancer Decedents' Hospital End-of-Life Care Documentation: A Retrospective Review of Patient Records.","authors":"L Russell, R Howard, M Street, C E Johnson, D Berry, E Flemming-Judge, S Brean, L William, J Considine","doi":"10.1177/08258597231170836","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objective:</b> International standards of end-of-life care (EOLC) intend to guide the delivery of safe and high-quality EOLC. Adequately documented care is conducive to higher quality of care, but the extent to which EOLC standards are documented in hospital medical records is unknown. Assessing which EOLC standards are documented in patients' medical records can help identify areas that are performed well and areas where improvements are needed. This study assessed cancer decedents' EOLC documentation in hospital settings. <b>Methods:</b> Medical records of 240 cancer decedents were retrospectively evaluated. Data were collected across six Australian hospitals between 1/01/2019 and 31/12/2019. EOLC documentation related to Advance Care Planning (ACP), resuscitation planning, care of the dying person, and grief and bereavement care was reviewed. Chi-square tests assessed associations between EOLC documentation and patient characteristics, and hospital settings (specialist palliative care unit, sub-acute/rehabilitation care settings, acute care wards, and intensive care units). <b>Results:</b> Decedents' mean age was 75.3 years (SD 11.8), 52.0% (n = 125) were female, and 73.7% lived with other adults or carers. All patients (n = 240; 100%) had documentation for resuscitation planning, 97.6% (n = 235) for Care for the Dying Person, 40.0% for grief and bereavement care (n = 96), and 30.4% (n = 73) for ACP. Patients living with other adults or carers were less likely to have a documented ACP than those living alone or with dependents (OR 0.48; 95% CI 0.26-0.89). EOLC documentation was significantly greater in specialist palliative care settings than that in other hospital settings (<i>P</i> < .001). <b>Conclusion:</b> The process of dying is well documented among inpatients diagnosed with cancer. ACP and grief and bereavement support are not documented enough. Organizational endorsement of a clear practice framework and increased training could improve documentation of these aspects of EOLC.</p>","PeriodicalId":51096,"journal":{"name":"Journal of Palliative Care","volume":" ","pages":"168-175"},"PeriodicalIF":1.7000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11967109/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Palliative Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/08258597231170836","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/4/27 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
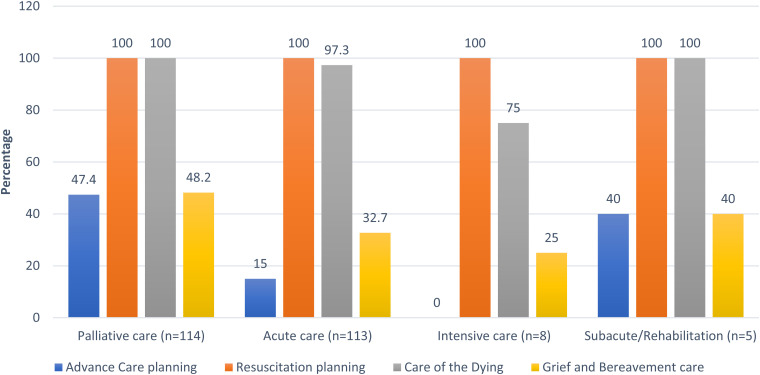
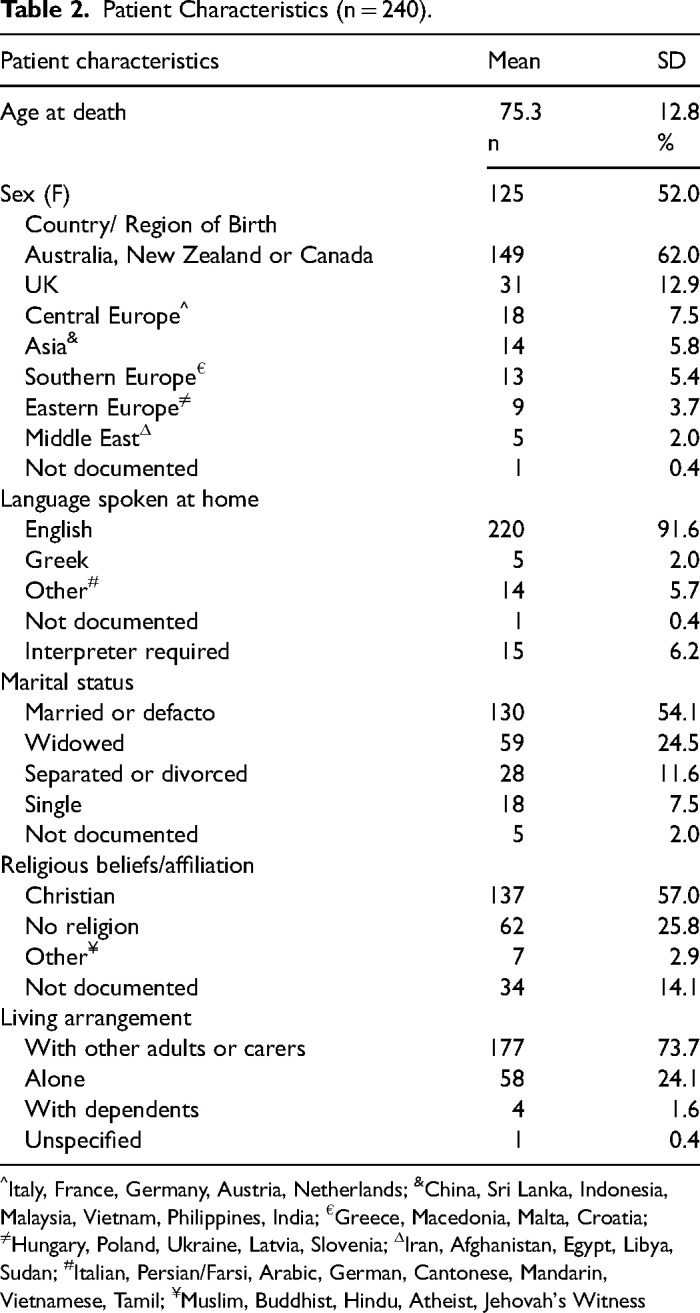
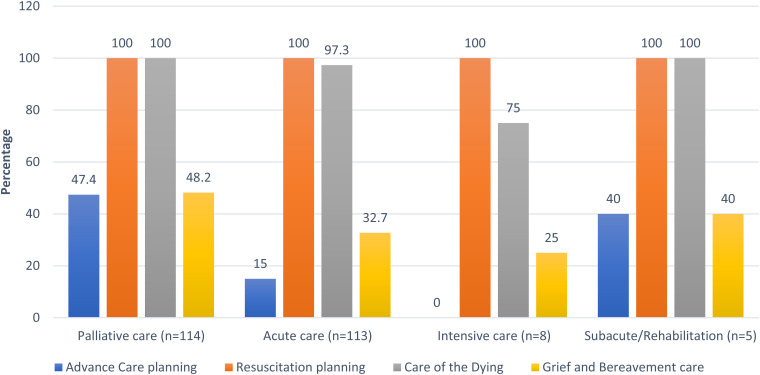
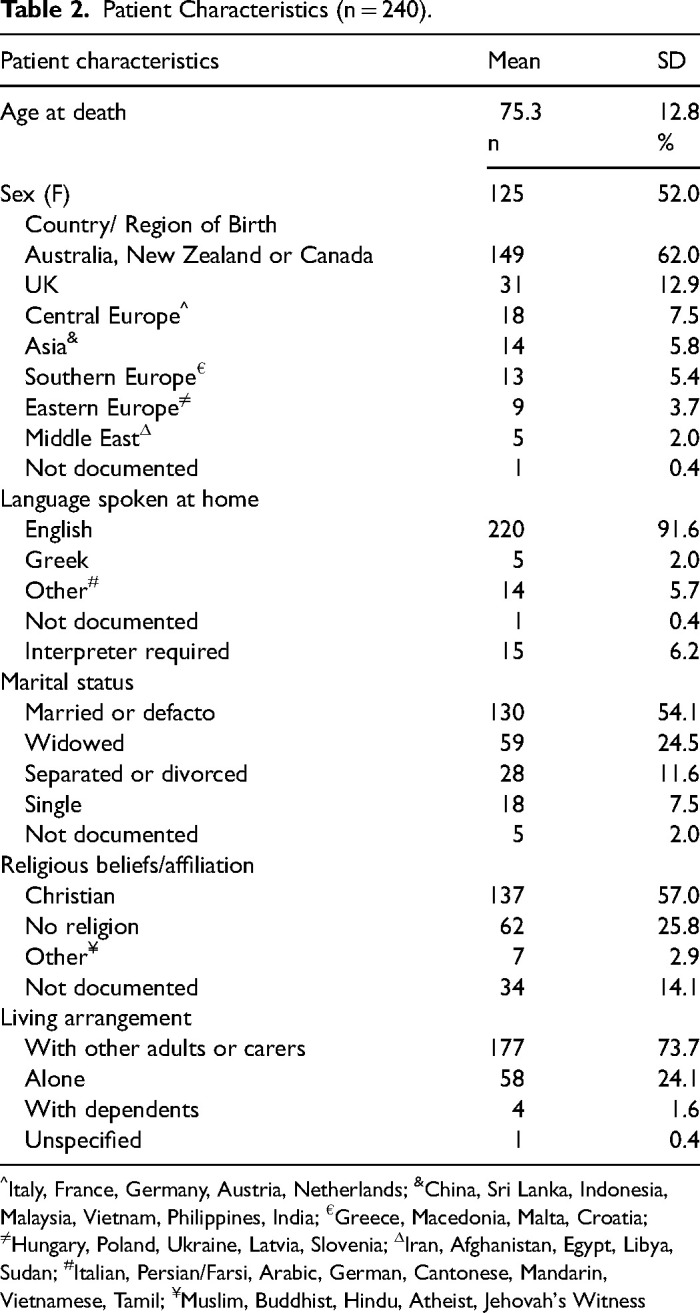
Objective: International standards of end-of-life care (EOLC) intend to guide the delivery of safe and high-quality EOLC. Adequately documented care is conducive to higher quality of care, but the extent to which EOLC standards are documented in hospital medical records is unknown. Assessing which EOLC standards are documented in patients' medical records can help identify areas that are performed well and areas where improvements are needed. This study assessed cancer decedents' EOLC documentation in hospital settings. Methods: Medical records of 240 cancer decedents were retrospectively evaluated. Data were collected across six Australian hospitals between 1/01/2019 and 31/12/2019. EOLC documentation related to Advance Care Planning (ACP), resuscitation planning, care of the dying person, and grief and bereavement care was reviewed. Chi-square tests assessed associations between EOLC documentation and patient characteristics, and hospital settings (specialist palliative care unit, sub-acute/rehabilitation care settings, acute care wards, and intensive care units). Results: Decedents' mean age was 75.3 years (SD 11.8), 52.0% (n = 125) were female, and 73.7% lived with other adults or carers. All patients (n = 240; 100%) had documentation for resuscitation planning, 97.6% (n = 235) for Care for the Dying Person, 40.0% for grief and bereavement care (n = 96), and 30.4% (n = 73) for ACP. Patients living with other adults or carers were less likely to have a documented ACP than those living alone or with dependents (OR 0.48; 95% CI 0.26-0.89). EOLC documentation was significantly greater in specialist palliative care settings than that in other hospital settings (P < .001). Conclusion: The process of dying is well documented among inpatients diagnosed with cancer. ACP and grief and bereavement support are not documented enough. Organizational endorsement of a clear practice framework and increased training could improve documentation of these aspects of EOLC.
期刊介绍:
The Journal of Palliative Care is a quarterly, peer-reviewed, international and interdisciplinary forum for practical, critical thought on palliative care and palliative medicine. JPC publishes high-quality original research, opinion papers/commentaries, narrative and humanities works, case reports/case series, and reports on international activities and comparative palliative care.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
