The Role of Frailty and Sarcopenia in Predicting Major Adverse Events, Length of Stay and Reoperation Following En Bloc Resection of Primary Tumours of the Spine.
Eryck Moskven, Oliver Lasry, Supriya Singh, Alana M Flexman, John T Street, Nicolas Dea, Charles G Fisher, Tamir Ailon, Marcel F Dvorak, Brian K Kwon, Scott J Paquette, Raphaële Charest-Morin
{"title":"The Role of Frailty and Sarcopenia in Predicting Major Adverse Events, Length of Stay and Reoperation Following <i>En Bloc</i> Resection of Primary Tumours of the Spine.","authors":"Eryck Moskven, Oliver Lasry, Supriya Singh, Alana M Flexman, John T Street, Nicolas Dea, Charles G Fisher, Tamir Ailon, Marcel F Dvorak, Brian K Kwon, Scott J Paquette, Raphaële Charest-Morin","doi":"10.1177/21925682231173360","DOIUrl":null,"url":null,"abstract":"<p><strong>Study design: </strong>Retrospective observational cohort study.</p><p><strong>Objective: </strong><i>En bloc</i> resection for primary tumours of the spine is associated with a high rate of adverse events (AEs). The objective was to explore the relationship between frailty/sarcopenia and major perioperative AEs, length of stay (LOS), and unplanned reoperation following <i>en bloc</i> resection of primary spinal tumours.</p><p><strong>Methods: </strong>This is a unicentre study consisting of adult patients undergoing <i>en bloc</i> resection for a primary spine tumor. Frailty was calculated with the modified frailty index (mFI) and spine tumour frailty index (STFI). Sarcopenia was quantified with the total psoas area/vertebral body area ratio (TPA/VB) at L3 and L4. Univariable regression analysis was used to quantify the association between frailty/sarcopenia and major perioperative AEs, LOS and unplanned reoperation.</p><p><strong>Results: </strong>95 patients met the inclusion criteria. The mFI and STFI identified a frailty prevalence of 3% and 18%. Mean CT TPA/VB ratios were 1.47 (SD ± .05) and 1.83 (SD ± .06) at L3 and L4. Inter-observer reliability was .93 and .99 for CT and MRI L3 and L4 TPA/VB ratios. Unadjusted analysis demonstrated sarcopenia and mFI did not predict perioperative AEs, LOS or unplanned reoperation. Frailty defined by an STFI score ≥2 predicted unplanned reoperation for surgical site infection (SSI) (<i>P</i> < .05).</p><p><strong>Conclusions: </strong>The STFI was only associated with unplanned reoperation for SSI on unadjusted analysis, while the mFI and sarcopenia were not predictive of any outcome. Further studies are needed to investigate the relationship between frailty, sarcopenia and perioperative outcomes following <i>en bloc</i> resection of primary spinal tumors.</p>","PeriodicalId":12680,"journal":{"name":"Global Spine Journal","volume":" ","pages":"2259-2269"},"PeriodicalIF":3.0000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11531018/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Spine Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/21925682231173360","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/4/28 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Study design: Retrospective observational cohort study.
Objective: En bloc resection for primary tumours of the spine is associated with a high rate of adverse events (AEs). The objective was to explore the relationship between frailty/sarcopenia and major perioperative AEs, length of stay (LOS), and unplanned reoperation following en bloc resection of primary spinal tumours.
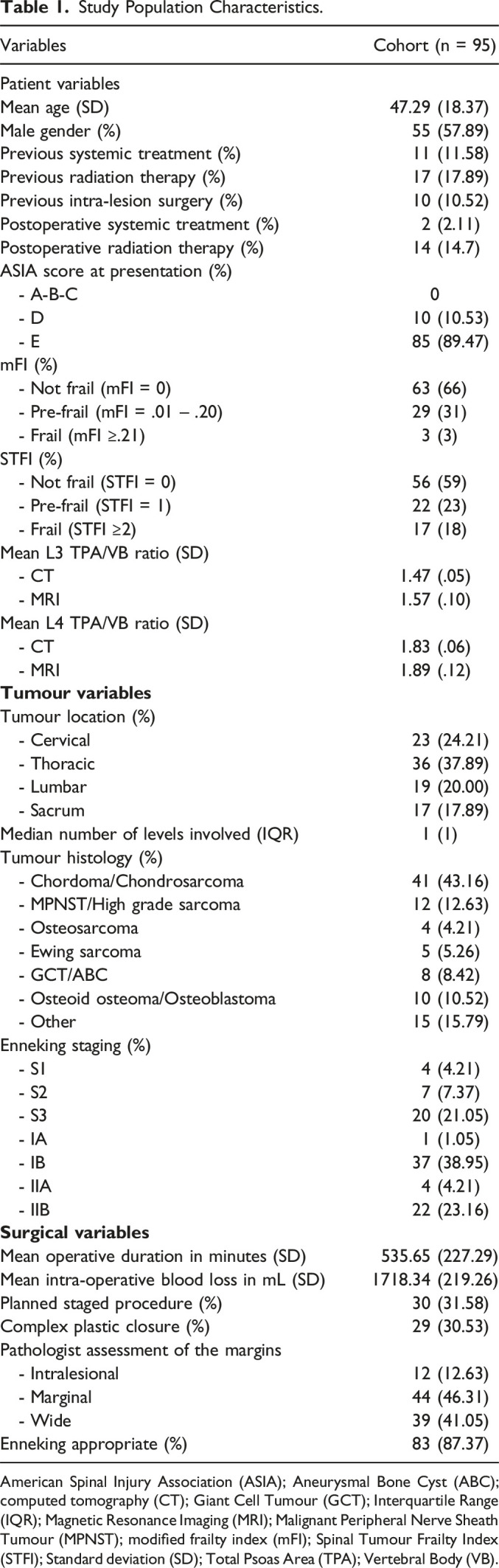
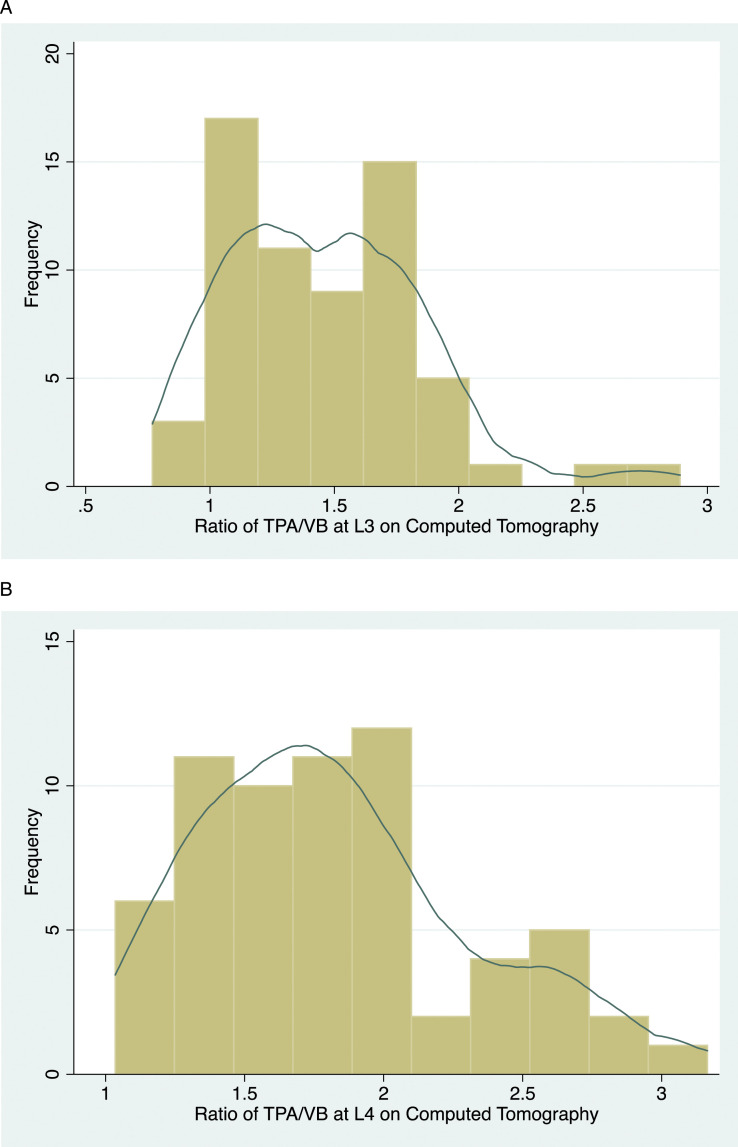
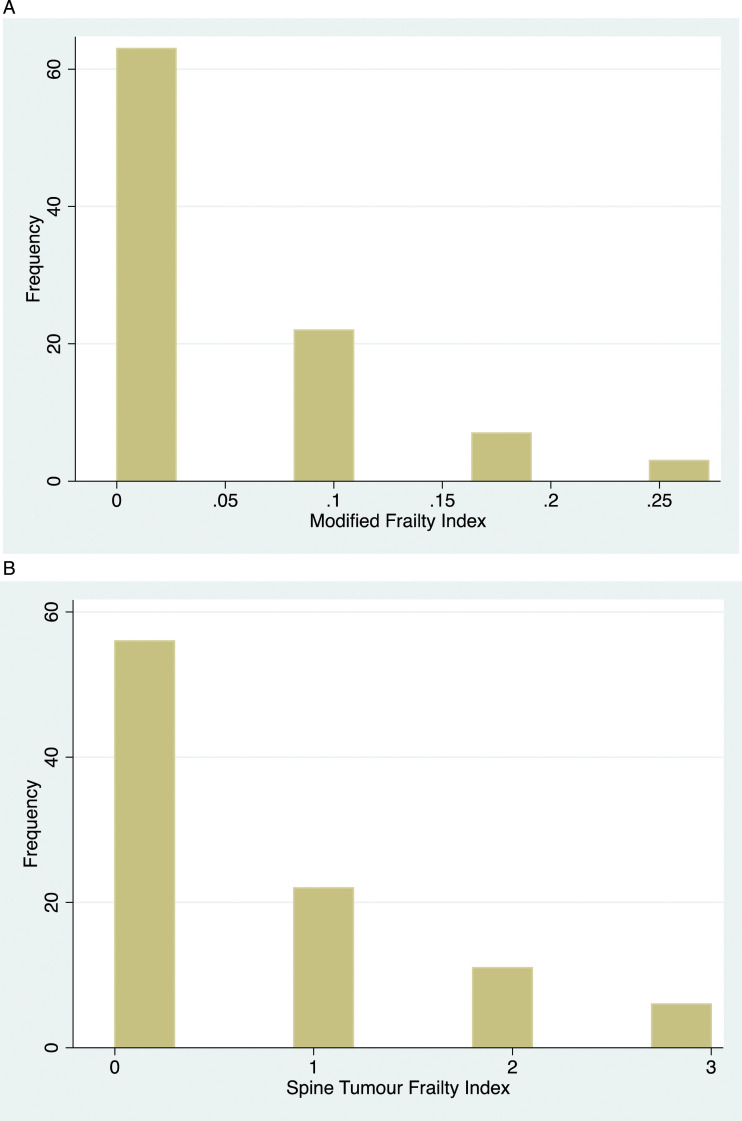
Methods: This is a unicentre study consisting of adult patients undergoing en bloc resection for a primary spine tumor. Frailty was calculated with the modified frailty index (mFI) and spine tumour frailty index (STFI). Sarcopenia was quantified with the total psoas area/vertebral body area ratio (TPA/VB) at L3 and L4. Univariable regression analysis was used to quantify the association between frailty/sarcopenia and major perioperative AEs, LOS and unplanned reoperation.
Results: 95 patients met the inclusion criteria. The mFI and STFI identified a frailty prevalence of 3% and 18%. Mean CT TPA/VB ratios were 1.47 (SD ± .05) and 1.83 (SD ± .06) at L3 and L4. Inter-observer reliability was .93 and .99 for CT and MRI L3 and L4 TPA/VB ratios. Unadjusted analysis demonstrated sarcopenia and mFI did not predict perioperative AEs, LOS or unplanned reoperation. Frailty defined by an STFI score ≥2 predicted unplanned reoperation for surgical site infection (SSI) (P < .05).
Conclusions: The STFI was only associated with unplanned reoperation for SSI on unadjusted analysis, while the mFI and sarcopenia were not predictive of any outcome. Further studies are needed to investigate the relationship between frailty, sarcopenia and perioperative outcomes following en bloc resection of primary spinal tumors.
期刊介绍:
Global Spine Journal (GSJ) is the official scientific publication of AOSpine. A peer-reviewed, open access journal, devoted to the study and treatment of spinal disorders, including diagnosis, operative and non-operative treatment options, surgical techniques, and emerging research and clinical developments.GSJ is indexed in PubMedCentral, SCOPUS, and Emerging Sources Citation Index (ESCI).



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
