Daniele Trombetti, Calogera Pisano, Maria Sabrina Ferrante, Laura Asta, Claudia Altieri, Paolo Nardi, Dario Buioni, Giovanni Ruvolo
{"title":"Cardiac angiosarcoma: a formidable challenge.","authors":"Daniele Trombetti, Calogera Pisano, Maria Sabrina Ferrante, Laura Asta, Claudia Altieri, Paolo Nardi, Dario Buioni, Giovanni Ruvolo","doi":"10.5114/kitp.2023.126101","DOIUrl":null,"url":null,"abstract":"Address for correspondence: Daniele Trombetti MD, Department of Cardiac Surgery, University of Tor Vergata, Rome, Italy, e-mail: daniele.trombetti@famigliatrombetti.it Received: 2.10.2022, accepted: 6.02.2023. Primary cardiac angiosarcoma (AS) is a clinically rare (incidence of about 0.017%) and highly invasive cardiac tumor with an unfavorable prognosis. The general prognosis of patients with primary cardiac sarcoma is poor, with median overall survival which ranges from 9 to 27 months in recent case series [1]. Cases of primary cardiac angiosarcoma (PCAS) are extraordinarily rare but represent most cases of malignant cardiac cancer. PCAS originates from vascular endothelial cells or vascular endothelial cells that have differentiated from mesenteric cells. Much of the literature indicates that a majority of PCAS cases occur in the right atrium. Cardiac sarcomas usually present insidious symptoms in young and middle-aged patients. They generally have an unfavorable prognosis with an overall survival of between 6 and 12 months. The treatment of choice for these rare malignancies is a combination of surgical resection and radioand/or chemotherapy [2]. However, in most cases, and in contrast to benign cardiac tumors, surgical resection still represents a palliative strategy for many patients with cardiac sarcomas. Therefore, rapid and accurate diagnosis is necessary and can confer a survival advantage on individual patients [3]. We report our experience with a young patient treated in our unit for an undifferentiated pleomorphic sarcoma who is still alive. As this study was carried out in order to improve the management of primary cardiac angiosarcoma, local approval at the level of the surgical department was obtained prior to data collection and the patient signed the consent form for scientific purposes. In April 2020, a 41-year-old patient was admitted to the Emergency Room of Tor Vergata University for dyspnea associated with chest tightness and vertigo. The echocardiography examination showed a round-shaped hyperechoic formation (6 × 4 cm) occupying all the left atrium until the inflow tract of the left ventricle with a large base of implantation in the anterior portion of the atrial septum (Figures 1 A–C). This mass engaged the mitral valve, resulting in severe steno-insufficiency (transvalvular medium gradient 27 mm Hg). A computed tomography (CT) raised the hypothesis of a PCAS (Figures 2 A–C). After a multidisciplinary clinical discussion, the patient was transferred to our Cardiac Surgery Unit for a cardiac operation. A standard longitudinal sternotomy was performed and the patient underwent cardiopulmonary bypass for exeresis of the mass. At the opening of the left atrium the mass adhered tenaciously to the atrial septum, the left auricle, the free wall of the left atrium and the anterior flap of the mitral valve. Despite the presence of tenacious adhesions of the mass to the atrial structures, it was possible to perform a total mass exeresis removing the atrial endocardium and mitral valve. We replaced the mitral valve with a Bicarbon Fitline mechanical prosthesis 25 mm. At the macroscopic examination the mass appeared bi-lobed, with a lardaceous consistency and a gray color. Histological examination evidenced a malignant mesenchymal neoplasm with spindle cells and necrotic areas associated with a severe inflammatory lympho-plasmacellular component. These findings confirmed an undifferentiated pleomorphic sarcoma. The postoperative course was uneventful and the patient was discharged on the 5th post-operative day. He immediately started a chemotherapy protocol with paclitaxel 150 mg/m2 in a 3 weeks on/1 week off regimen and propranolol 40 mg three times daily associated with a moderate dose of radiotherapy of the chest. Two years’ follow-up showed no recurrence of pathology. He is still alive and in good health (Figures 3 A–E). Primary tumors of the heart are extremely rare, and the majority are benign. PCAS is the most common primary malignant tumor of the heart [4]. It is a rare subgroup of soft tissue sarcomas, and is associated with a poor prognosis due to its aggressive nature and high rates of local recurrence and systemic metastases [5]. The rapid infiltrating growth of this tumor can lead to emergency clinical presentations including pericardial effusions, cardiac tamponade, and myocardial rupture [6]. The treatment of choice for these rare malignancies is a combination of surgical resection and radioand/or chemotherapy. However, in most cases, and in contrast to benign cardiac tumors, surgical resection still represents a palliative strategy for many patients with cardiac sarcomas. An immediate diagnosis and quick treatment represent the only weapon to defeat this insidious disease, as we showed in this interesting case report. Several studies Cardiac angiosarcoma: a formidable challenge","PeriodicalId":49945,"journal":{"name":"Kardiochirurgia I Torakochirurgia Polska","volume":"20 1","pages":"53-56"},"PeriodicalIF":1.3000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b0/6e/KITP-20-50414.PMC10107413.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Kardiochirurgia I Torakochirurgia Polska","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/kitp.2023.126101","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
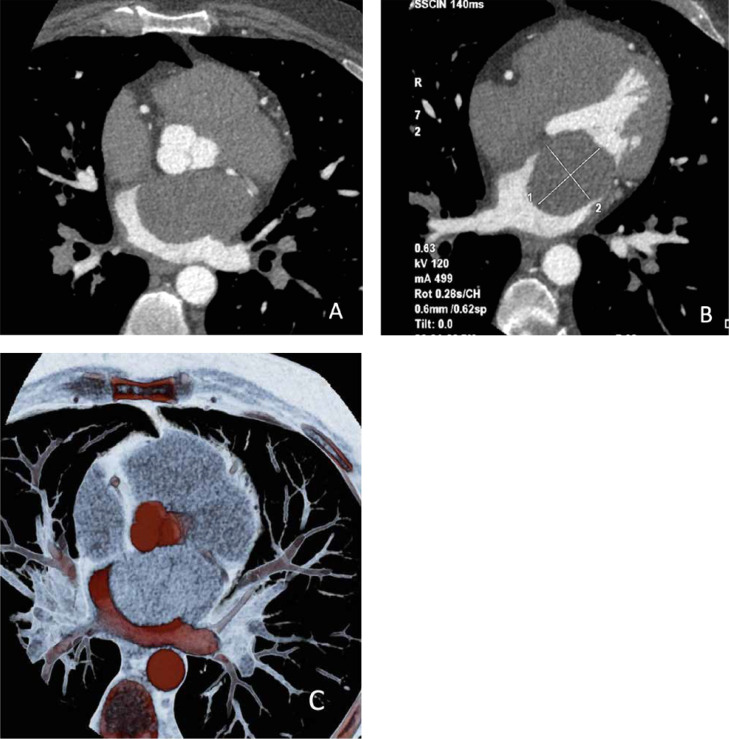
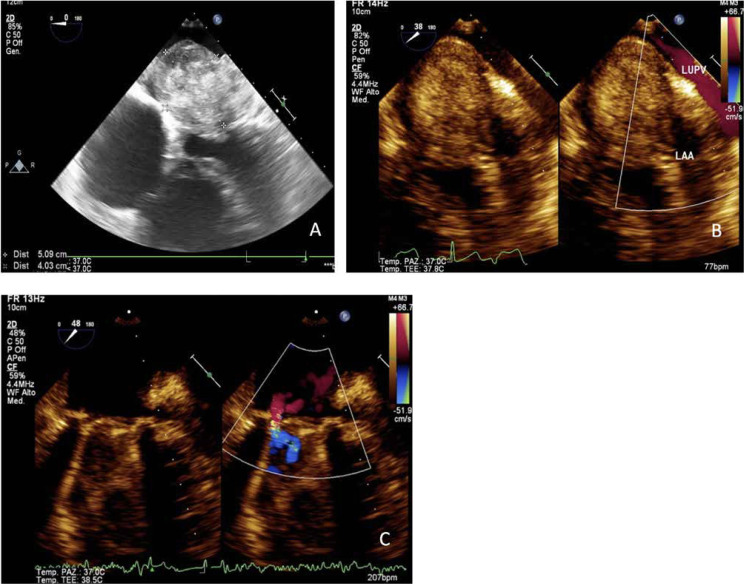
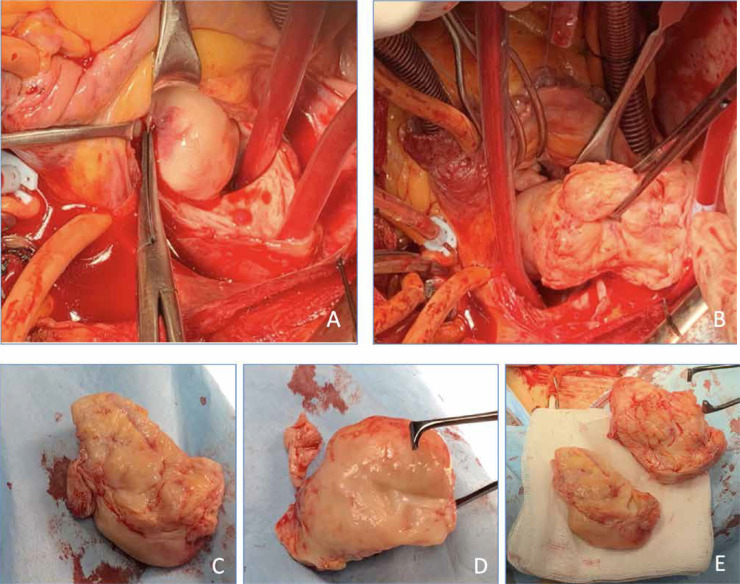
Address for correspondence: Daniele Trombetti MD, Department of Cardiac Surgery, University of Tor Vergata, Rome, Italy, e-mail: daniele.trombetti@famigliatrombetti.it Received: 2.10.2022, accepted: 6.02.2023. Primary cardiac angiosarcoma (AS) is a clinically rare (incidence of about 0.017%) and highly invasive cardiac tumor with an unfavorable prognosis. The general prognosis of patients with primary cardiac sarcoma is poor, with median overall survival which ranges from 9 to 27 months in recent case series [1]. Cases of primary cardiac angiosarcoma (PCAS) are extraordinarily rare but represent most cases of malignant cardiac cancer. PCAS originates from vascular endothelial cells or vascular endothelial cells that have differentiated from mesenteric cells. Much of the literature indicates that a majority of PCAS cases occur in the right atrium. Cardiac sarcomas usually present insidious symptoms in young and middle-aged patients. They generally have an unfavorable prognosis with an overall survival of between 6 and 12 months. The treatment of choice for these rare malignancies is a combination of surgical resection and radioand/or chemotherapy [2]. However, in most cases, and in contrast to benign cardiac tumors, surgical resection still represents a palliative strategy for many patients with cardiac sarcomas. Therefore, rapid and accurate diagnosis is necessary and can confer a survival advantage on individual patients [3]. We report our experience with a young patient treated in our unit for an undifferentiated pleomorphic sarcoma who is still alive. As this study was carried out in order to improve the management of primary cardiac angiosarcoma, local approval at the level of the surgical department was obtained prior to data collection and the patient signed the consent form for scientific purposes. In April 2020, a 41-year-old patient was admitted to the Emergency Room of Tor Vergata University for dyspnea associated with chest tightness and vertigo. The echocardiography examination showed a round-shaped hyperechoic formation (6 × 4 cm) occupying all the left atrium until the inflow tract of the left ventricle with a large base of implantation in the anterior portion of the atrial septum (Figures 1 A–C). This mass engaged the mitral valve, resulting in severe steno-insufficiency (transvalvular medium gradient 27 mm Hg). A computed tomography (CT) raised the hypothesis of a PCAS (Figures 2 A–C). After a multidisciplinary clinical discussion, the patient was transferred to our Cardiac Surgery Unit for a cardiac operation. A standard longitudinal sternotomy was performed and the patient underwent cardiopulmonary bypass for exeresis of the mass. At the opening of the left atrium the mass adhered tenaciously to the atrial septum, the left auricle, the free wall of the left atrium and the anterior flap of the mitral valve. Despite the presence of tenacious adhesions of the mass to the atrial structures, it was possible to perform a total mass exeresis removing the atrial endocardium and mitral valve. We replaced the mitral valve with a Bicarbon Fitline mechanical prosthesis 25 mm. At the macroscopic examination the mass appeared bi-lobed, with a lardaceous consistency and a gray color. Histological examination evidenced a malignant mesenchymal neoplasm with spindle cells and necrotic areas associated with a severe inflammatory lympho-plasmacellular component. These findings confirmed an undifferentiated pleomorphic sarcoma. The postoperative course was uneventful and the patient was discharged on the 5th post-operative day. He immediately started a chemotherapy protocol with paclitaxel 150 mg/m2 in a 3 weeks on/1 week off regimen and propranolol 40 mg three times daily associated with a moderate dose of radiotherapy of the chest. Two years’ follow-up showed no recurrence of pathology. He is still alive and in good health (Figures 3 A–E). Primary tumors of the heart are extremely rare, and the majority are benign. PCAS is the most common primary malignant tumor of the heart [4]. It is a rare subgroup of soft tissue sarcomas, and is associated with a poor prognosis due to its aggressive nature and high rates of local recurrence and systemic metastases [5]. The rapid infiltrating growth of this tumor can lead to emergency clinical presentations including pericardial effusions, cardiac tamponade, and myocardial rupture [6]. The treatment of choice for these rare malignancies is a combination of surgical resection and radioand/or chemotherapy. However, in most cases, and in contrast to benign cardiac tumors, surgical resection still represents a palliative strategy for many patients with cardiac sarcomas. An immediate diagnosis and quick treatment represent the only weapon to defeat this insidious disease, as we showed in this interesting case report. Several studies Cardiac angiosarcoma: a formidable challenge
期刊介绍:
Polish Journal of Thoracic and Cardiovascular Surgery is a quarterly aimed at cardiologists, cardiosurgeons and thoracic surgeons. Includes the original works (experimental, research and development), illustrative and casuistical works about cardiology and cardiosurgery.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
