Madeline S Tiee, Andrew G Golz, Andrew Kim, Joseph B Cohen, Hobie D Summers, Anup J Alexander, William D Lack
{"title":"Sagittal deformity of Garden type I and II geriatric femoral neck fractures is frequently misclassified by lateral radiographs.","authors":"Madeline S Tiee, Andrew G Golz, Andrew Kim, Joseph B Cohen, Hobie D Summers, Anup J Alexander, William D Lack","doi":"10.1097/OI9.0000000000000273","DOIUrl":null,"url":null,"abstract":"<p><p>The objective of this study was to determine the validity and inter-rater reliability of radiographic assessment of sagittal deformity of femoral neck fractures.</p><p><strong>Design: </strong>This is a retrospective cohort study.</p><p><strong>Setting: </strong>Level 1 trauma center.</p><p><strong>Patients/participants: </strong>Thirty-one patients 65 years or older who sustained low-energy, Garden type I/II femoral neck fractures imaged with biplanar radiographs and either computed tomography or magnetic resonance imaging were included.</p><p><strong>Main outcome measurements: </strong>Preoperative sagittal tilt was measured on lateral radiographs and compared with the tilt identified on advanced imaging. Fractures were defined as \"high-risk\" if posterior tilt was ≥20 degrees or anterior tilt was >10 degrees.</p><p><strong>Results: </strong>Of 31 Garden type I/II femoral neck fractures, advanced imaging identified 10 high-risk fractures including 8 (25.8%) with posterior tilt ≥20 degrees and 2 (6.5%) with anterior tilt >10 degrees. Overall, there was no significant difference between sagittal tilt measured using lateral radiographs and advanced imaging (<i>P</i> = 0.84), and the 3 raters had good agreement between their measurements of sagittal tilt on lateral radiographs (interclass correlation coefficient 0.79, 95% confidence interval [0.65, 0.88], <i>P</i> < 0.01). However, for high-risk fractures, radiographic measurements from lateral radiographs alone resulted in greater variability and underestimation of tilt by 5.2 degrees (95% confidence interval [-18.68, 8.28]) when compared with computed tomography/magnetic resonance imaging. Owing to this underestimation of sagittal tilt, the raters misclassified high-risk fractures as \"low-risk\" in most cases (averaging 6.3 of 10, 63%, range 6 - 7) when using lateral radiographs while low-risk fractures were rarely misclassified as high-risk (averaging 1.7 of 21, 7.9%, range 1 - 3, <i>P</i> = 0.01).</p><p><strong>Conclusions: </strong>Lateral radiographs frequently lead surgeons to misclassify high-risk sagittal tilt of low-energy femoral neck fractures as low-risk. Further research is necessary to improve the assessment of sagittal plane deformity for these injuries.</p><p><strong>Level of evidence: </strong>Level IV diagnostic study.</p>","PeriodicalId":74381,"journal":{"name":"OTA international : the open access journal of orthopaedic trauma","volume":"6 2","pages":"e273"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f6/e7/oi9-6-e273.PMC10113109.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"OTA international : the open access journal of orthopaedic trauma","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/OI9.0000000000000273","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
The objective of this study was to determine the validity and inter-rater reliability of radiographic assessment of sagittal deformity of femoral neck fractures.
Design: This is a retrospective cohort study.
Setting: Level 1 trauma center.
Patients/participants: Thirty-one patients 65 years or older who sustained low-energy, Garden type I/II femoral neck fractures imaged with biplanar radiographs and either computed tomography or magnetic resonance imaging were included.
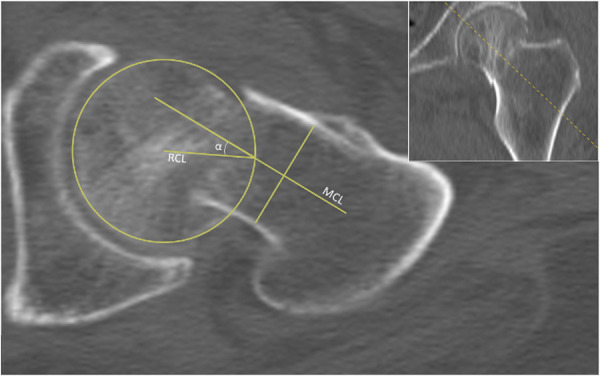
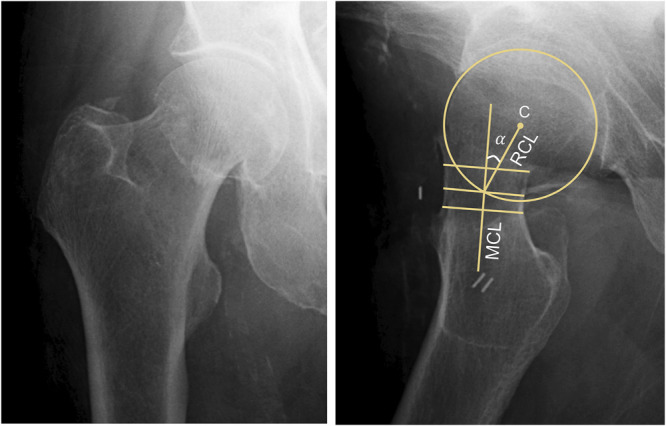
Main outcome measurements: Preoperative sagittal tilt was measured on lateral radiographs and compared with the tilt identified on advanced imaging. Fractures were defined as "high-risk" if posterior tilt was ≥20 degrees or anterior tilt was >10 degrees.
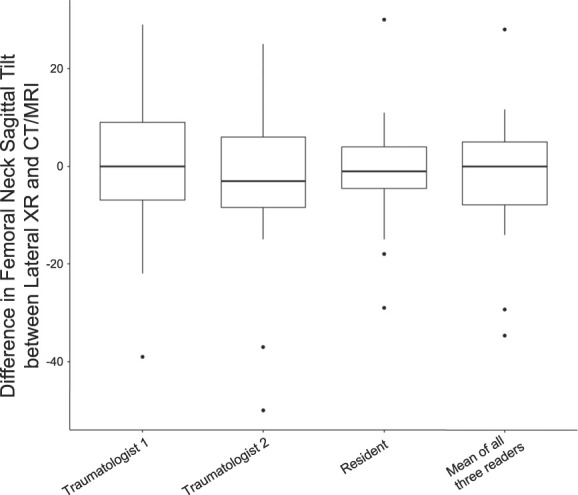
Results: Of 31 Garden type I/II femoral neck fractures, advanced imaging identified 10 high-risk fractures including 8 (25.8%) with posterior tilt ≥20 degrees and 2 (6.5%) with anterior tilt >10 degrees. Overall, there was no significant difference between sagittal tilt measured using lateral radiographs and advanced imaging (P = 0.84), and the 3 raters had good agreement between their measurements of sagittal tilt on lateral radiographs (interclass correlation coefficient 0.79, 95% confidence interval [0.65, 0.88], P < 0.01). However, for high-risk fractures, radiographic measurements from lateral radiographs alone resulted in greater variability and underestimation of tilt by 5.2 degrees (95% confidence interval [-18.68, 8.28]) when compared with computed tomography/magnetic resonance imaging. Owing to this underestimation of sagittal tilt, the raters misclassified high-risk fractures as "low-risk" in most cases (averaging 6.3 of 10, 63%, range 6 - 7) when using lateral radiographs while low-risk fractures were rarely misclassified as high-risk (averaging 1.7 of 21, 7.9%, range 1 - 3, P = 0.01).
Conclusions: Lateral radiographs frequently lead surgeons to misclassify high-risk sagittal tilt of low-energy femoral neck fractures as low-risk. Further research is necessary to improve the assessment of sagittal plane deformity for these injuries.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
