Carlin P Hoffacker, Melanie Klein, Emily M Becker-Haimes, Jessica Fishman, Sonja K Schoenwald, Perrin B Fugo, Bryce D McLeod, Shannon Dorsey, Shannon Litke, Lah'Nasia Shider, Adina Lieberman, David S Mandell, Rinad S Beidas
{"title":"Stakeholder intention to engage in fidelity measurement methods in community mental health settings: A mixed methods study.","authors":"Carlin P Hoffacker, Melanie Klein, Emily M Becker-Haimes, Jessica Fishman, Sonja K Schoenwald, Perrin B Fugo, Bryce D McLeod, Shannon Dorsey, Shannon Litke, Lah'Nasia Shider, Adina Lieberman, David S Mandell, Rinad S Beidas","doi":"10.1177/26334895221114664","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The current gold standard for measuring fidelity (specifically, adherence) to cognitive behavioral therapy (CBT) is direct observation, a costly, resource-intensive practice that is not feasible for many community organizations to implement regularly. Recent research indicates that behavioral rehearsal (i.e., role-play between clinician and individual with regard to session delivery) and chart-stimulated recall (i.e., brief structured interview between clinician and individual about what they did in session; clinicians use the client chart to prompt memory) may provide accurate and affordable alternatives for measuring adherence to CBT in such settings, with behavioral rehearsal yielding greater correspondence with direct observation.</p><p><strong>Methods: </strong>Drawing on established causal theories from social psychology and leading implementation science frameworks, this study evaluates stakeholders' intention to use behavioral rehearsal and chart-stimulated recall. Specifically, we measured attitudes, self-efficacy, and subjective norms toward using each, and compared these factors across the two methods. We also examined the relationship between attitudes, self-efficacy, subjective norms, and intention to use each method. Finally, using an integrated approach we asked stakeholders to discuss their perception of contextual factors that may influence beliefs about using each method. These data were collected from community-based supervisors (<i>n</i> = 17) and clinicians (<i>n</i> = 66).</p><p><strong>Results: </strong>Quantitative analyses suggest moderately strong intention to use both methods across stakeholders. There were no differences in supervisors' or clinicians' attitudes, self-efficacy, subjective norms, or intention across methods. More positive attitudes and greater reported subjective norms were associated with greater reported intention to use either measure. Qualitative analyses identified participants' specific beliefs about using each fidelity measure in their organization, and results were organized using the Consolidated Framework for Implementation Research.</p><p><strong>Conclusions: </strong>Strategies are warranted to overcome or minimize potential barriers to using fidelity measurement methods and to further increase the strength of intention to use them.<b>Plain Language Summary:</b> The best way to measure fidelity, or how closely a clinician follows the protocol, to Cognitive Behavioral Therapy (CBT) is watching the session. This is an expensive practice that is not feasible for many community organizations to do regularly. Recent research indicates that behavioral rehearsal, or a role-play between the clinician and individual with regard to session delivery, and chart-stimulated recall, or a brief discussion between an individual and the clinician about what they did in session with the clinician having access to the chart to help them remember, may provide accurate and affordable alternatives for measuring fidelity to CBT. We just completed a study demonstrating that both methods are promising, with behavioral rehearsal offering scores that are the most similar to watching the session. Drawing on established theories from social psychology and leading implementation science frameworks, this study evaluates future supervisor and clinician motivation to use these fidelity measurement methods. Specifically, we measured supervisor (n = 17) and clinician (n = 66) attitudes, norms, self-efficacy, intentions, and anticipated barriers and facilitators to using each of these fidelity measurement tools. Quantitative and qualitative analyses suggest similar intention to use both methods, and concerns about barriers to using each method. Further research is warranted to minimize the burden associated with implementing fidelity measurement methods and deploying strategies to increase use.</p>","PeriodicalId":73354,"journal":{"name":"Implementation research and practice","volume":"3 ","pages":"26334895221114664"},"PeriodicalIF":2.6000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0b/d4/10.1177_26334895221114664.PMC9924256.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26334895221114664","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The current gold standard for measuring fidelity (specifically, adherence) to cognitive behavioral therapy (CBT) is direct observation, a costly, resource-intensive practice that is not feasible for many community organizations to implement regularly. Recent research indicates that behavioral rehearsal (i.e., role-play between clinician and individual with regard to session delivery) and chart-stimulated recall (i.e., brief structured interview between clinician and individual about what they did in session; clinicians use the client chart to prompt memory) may provide accurate and affordable alternatives for measuring adherence to CBT in such settings, with behavioral rehearsal yielding greater correspondence with direct observation.
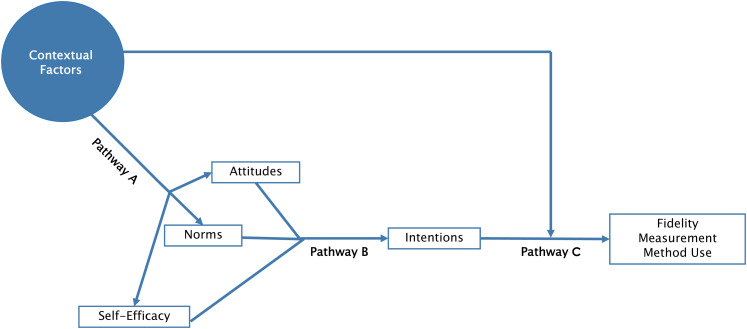
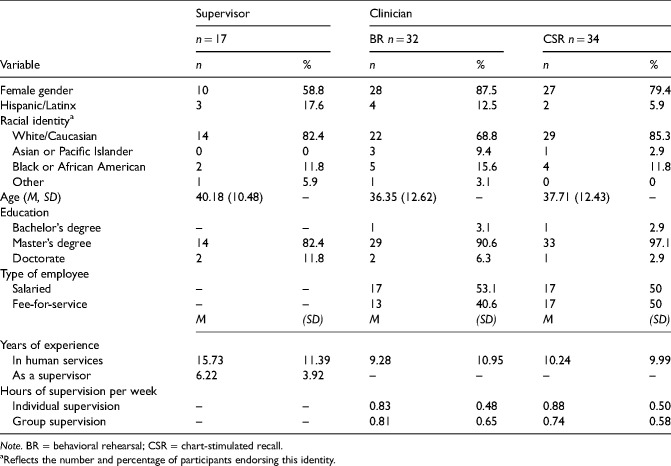
Methods: Drawing on established causal theories from social psychology and leading implementation science frameworks, this study evaluates stakeholders' intention to use behavioral rehearsal and chart-stimulated recall. Specifically, we measured attitudes, self-efficacy, and subjective norms toward using each, and compared these factors across the two methods. We also examined the relationship between attitudes, self-efficacy, subjective norms, and intention to use each method. Finally, using an integrated approach we asked stakeholders to discuss their perception of contextual factors that may influence beliefs about using each method. These data were collected from community-based supervisors (n = 17) and clinicians (n = 66).
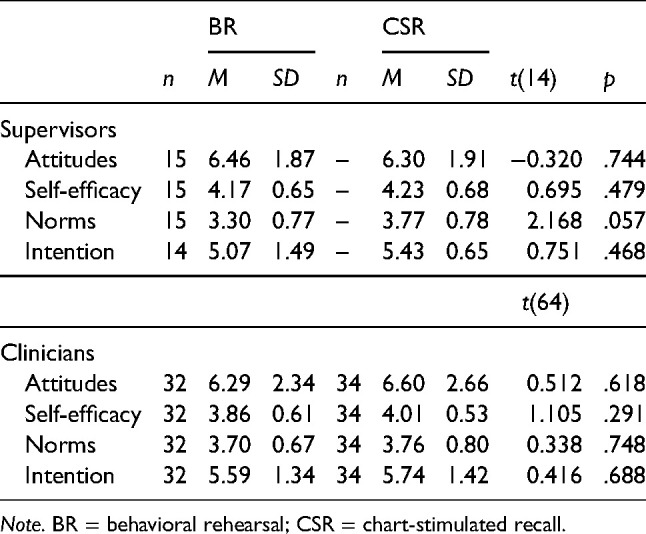
Results: Quantitative analyses suggest moderately strong intention to use both methods across stakeholders. There were no differences in supervisors' or clinicians' attitudes, self-efficacy, subjective norms, or intention across methods. More positive attitudes and greater reported subjective norms were associated with greater reported intention to use either measure. Qualitative analyses identified participants' specific beliefs about using each fidelity measure in their organization, and results were organized using the Consolidated Framework for Implementation Research.
Conclusions: Strategies are warranted to overcome or minimize potential barriers to using fidelity measurement methods and to further increase the strength of intention to use them.Plain Language Summary: The best way to measure fidelity, or how closely a clinician follows the protocol, to Cognitive Behavioral Therapy (CBT) is watching the session. This is an expensive practice that is not feasible for many community organizations to do regularly. Recent research indicates that behavioral rehearsal, or a role-play between the clinician and individual with regard to session delivery, and chart-stimulated recall, or a brief discussion between an individual and the clinician about what they did in session with the clinician having access to the chart to help them remember, may provide accurate and affordable alternatives for measuring fidelity to CBT. We just completed a study demonstrating that both methods are promising, with behavioral rehearsal offering scores that are the most similar to watching the session. Drawing on established theories from social psychology and leading implementation science frameworks, this study evaluates future supervisor and clinician motivation to use these fidelity measurement methods. Specifically, we measured supervisor (n = 17) and clinician (n = 66) attitudes, norms, self-efficacy, intentions, and anticipated barriers and facilitators to using each of these fidelity measurement tools. Quantitative and qualitative analyses suggest similar intention to use both methods, and concerns about barriers to using each method. Further research is warranted to minimize the burden associated with implementing fidelity measurement methods and deploying strategies to increase use.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
