Hanna Pihlaja, Heidi Rantala, Sirpa Leivo-Korpela, Lauri Lehtimäki, Juho T Lehto, Reetta P Piili
{"title":"Specialist Palliative Care Consultation for Patients with Nonmalignant Pulmonary Diseases: A Retrospective Study.","authors":"Hanna Pihlaja, Heidi Rantala, Sirpa Leivo-Korpela, Lauri Lehtimäki, Juho T Lehto, Reetta P Piili","doi":"10.1089/pmr.2022.0068","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Few patients with chronic nonmalignant pulmonary diseases receive specialist palliative care consultation, despite their high symptom burden in end of life.</p><p><strong>Objectives: </strong>To study palliative care decision making, survival, and hospital resource usage in patients with nonmalignant pulmonary diseases with or without a specialist palliative care consultation.</p><p><strong>Methods: </strong>A retrospective chart review of all patients with a chronic nonmalignant pulmonary disease and a palliative care decision (palliative goal of therapy), who were treated in Tampere University Hospital, Finland, between January 1, 2018 and December 31, 2020.</p><p><strong>Results: </strong>A total of 107 patients were included in the study, 62 (58%) had chronic obstructive pulmonary disease (COPD), and 43 (40%) interstitial lung disease (ILD). Median survival after palliative care decision was shorter in patients with ILD than in patients with COPD (59 vs. 213 days, <i>p</i> = 0.004). Involvement of a palliative care specialist in the decision making was not associated with the survival. Patients with COPD who received palliative care consultation visited less often emergency room (73% vs. 100%, <i>p</i> = 0.019) and spent fewer days in the hospital (7 vs. 18 days, <i>p</i> = 0.007) during the last year of life. When a palliative care specialist attended the decision making, the presence and opinions of the patients were recorded more often, and the patients were more frequently referred to a palliative care pathway.</p><p><strong>Conclusions: </strong>Specialist palliative care consultation seems to enable better end-of-life care and supports shared decision making for patients with nonmalignant pulmonary diseases. Therefore, palliative care consultations should be utilized in nonmalignant pulmonary diseases preferably before the last days of life.</p>","PeriodicalId":74394,"journal":{"name":"Palliative medicine reports","volume":"4 1","pages":"108-115"},"PeriodicalIF":1.3000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10122226/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Palliative medicine reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/pmr.2022.0068","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Few patients with chronic nonmalignant pulmonary diseases receive specialist palliative care consultation, despite their high symptom burden in end of life.
Objectives: To study palliative care decision making, survival, and hospital resource usage in patients with nonmalignant pulmonary diseases with or without a specialist palliative care consultation.
Methods: A retrospective chart review of all patients with a chronic nonmalignant pulmonary disease and a palliative care decision (palliative goal of therapy), who were treated in Tampere University Hospital, Finland, between January 1, 2018 and December 31, 2020.
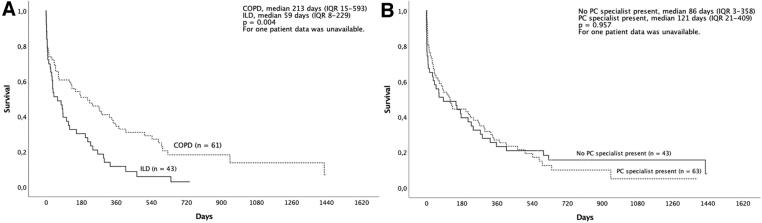
Results: A total of 107 patients were included in the study, 62 (58%) had chronic obstructive pulmonary disease (COPD), and 43 (40%) interstitial lung disease (ILD). Median survival after palliative care decision was shorter in patients with ILD than in patients with COPD (59 vs. 213 days, p = 0.004). Involvement of a palliative care specialist in the decision making was not associated with the survival. Patients with COPD who received palliative care consultation visited less often emergency room (73% vs. 100%, p = 0.019) and spent fewer days in the hospital (7 vs. 18 days, p = 0.007) during the last year of life. When a palliative care specialist attended the decision making, the presence and opinions of the patients were recorded more often, and the patients were more frequently referred to a palliative care pathway.
Conclusions: Specialist palliative care consultation seems to enable better end-of-life care and supports shared decision making for patients with nonmalignant pulmonary diseases. Therefore, palliative care consultations should be utilized in nonmalignant pulmonary diseases preferably before the last days of life.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
