"To Be or Not to Be"-Cardiopulmonary Resuscitation for Hospitalized People Who Have a Low Probability of Benefit: Qualitative Analysis of Semi-structured Interviews.
Daniel Kobewka, Yasmin Lalani, Victoria Shaffer, Tolulope Adewole, Kiefer Lypka, Pete Wegier
{"title":"\"To Be or Not to Be\"-Cardiopulmonary Resuscitation for Hospitalized People Who Have a Low Probability of Benefit: Qualitative Analysis of Semi-structured Interviews.","authors":"Daniel Kobewka, Yasmin Lalani, Victoria Shaffer, Tolulope Adewole, Kiefer Lypka, Pete Wegier","doi":"10.1177/23814683231168589","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Our aim was to understand the decision making of patients in hospital who wanted cardiopulmonary resuscitation despite low probability of benefit.</p><p><strong>Methods: </strong>We included patients admitted to general medical wards who had a low chance of surviving in-hospital cardiopulmonary resuscitation (CPR) and had an order in the chart to administer CPR. We developed an interview guide to explore participants' decision-making process, sources of information, and emotions associated with this decision.</p><p><strong>Results: </strong>We developed 3 themes from the data. 1) \"Life is worth living . . . for now\": Participants describe their enjoyment of life and desire to carry on in their current state. 2) \"Making sense of CPR outcomes\": Participants saw CPR outcomes as binary, either they live, or they die; deciding not to receive CPR means choosing death. Participants were optimistic they would survive CPR and cited personal experience and TV as information sources. 3) \"Decision process\": Participants did not engage in shared decision making. Instead, they were asked a binary yes/no question with no reflection on their values or discussion about harms or benefits.</p><p><strong>Limitations: </strong>The probability of successful CPR in our sample is unknown. Findings may be different in a population who is imminently dying but still requesting CPR.</p><p><strong>Conclusions: </strong>Participants chose CPR because they perceived life as worth living and CPR as a chance worth taking. Participants did not want to be left in a severely debilitated state but did not have accurate information about this risk.</p><p><strong>Implications: </strong>Decision making about CPR in-hospital can be improved if it is grounded in accurate risk understanding and the patient's values and wishes.</p>","PeriodicalId":36567,"journal":{"name":"MDM Policy and Practice","volume":"8 1","pages":"23814683231168589"},"PeriodicalIF":1.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d7/b7/10.1177_23814683231168589.PMC10141296.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"MDM Policy and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23814683231168589","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Our aim was to understand the decision making of patients in hospital who wanted cardiopulmonary resuscitation despite low probability of benefit.
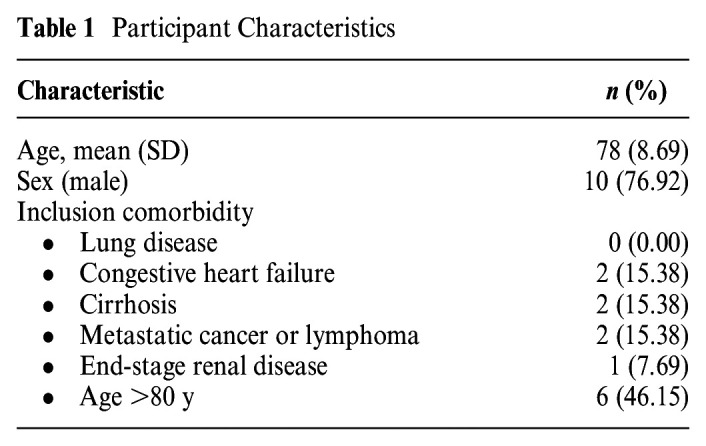
Methods: We included patients admitted to general medical wards who had a low chance of surviving in-hospital cardiopulmonary resuscitation (CPR) and had an order in the chart to administer CPR. We developed an interview guide to explore participants' decision-making process, sources of information, and emotions associated with this decision.
Results: We developed 3 themes from the data. 1) "Life is worth living . . . for now": Participants describe their enjoyment of life and desire to carry on in their current state. 2) "Making sense of CPR outcomes": Participants saw CPR outcomes as binary, either they live, or they die; deciding not to receive CPR means choosing death. Participants were optimistic they would survive CPR and cited personal experience and TV as information sources. 3) "Decision process": Participants did not engage in shared decision making. Instead, they were asked a binary yes/no question with no reflection on their values or discussion about harms or benefits.
Limitations: The probability of successful CPR in our sample is unknown. Findings may be different in a population who is imminently dying but still requesting CPR.
Conclusions: Participants chose CPR because they perceived life as worth living and CPR as a chance worth taking. Participants did not want to be left in a severely debilitated state but did not have accurate information about this risk.
Implications: Decision making about CPR in-hospital can be improved if it is grounded in accurate risk understanding and the patient's values and wishes.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
