Purity Njagi, Wim Groot, Jelena Arsenijevic, Silke Dyer, Gitau Mburu, James Kiarie
{"title":"Financial costs of assisted reproductive technology for patients in low- and middle-income countries: a systematic review.","authors":"Purity Njagi, Wim Groot, Jelena Arsenijevic, Silke Dyer, Gitau Mburu, James Kiarie","doi":"10.1093/hropen/hoad007","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>What are the direct costs of assisted reproductive technology (ART), and how affordable is it for patients in low- and middle-income countries (LMICS)?</p><p><strong>Summary answer: </strong>Direct medical costs paid by patients for infertility treatment are significantly higher than annual average income and GDP per capita, pointing to unaffordability and the risk of catastrophic expenditure for those in need.</p><p><strong>What is known already: </strong>Infertility treatment is largely inaccessible to many people in LMICs. Our analysis shows that no study in LMICs has previously compared ART medical costs across countries in international dollar terms (US$PPP) or correlated the medical costs with economic indicators, financing mechanisms, and policy regulations. Previous systematic reviews on costs have been limited to high-income countries while those in LMICs have only focussed on descriptive analyses of these costs.</p><p><strong>Study design size duration: </strong>Guided by the preferred reporting items for systematic reviews and meta-analyses (PRISMA), we searched PubMed, Web of Science, Cumulative Index of Nursing and Allied Health Literature, EconLit, PsycINFO, Latin American & Caribbean Health Sciences Literature, and grey literature for studies published in all languages from LMICs between 2001 and 2020.</p><p><strong>Participants/materials setting methods: </strong>The primary outcome of interest was direct medical costs paid by patients for one ART cycle. To gauge ART affordability, direct medical costs were correlated with the GDP per capita or average income of respective countries. ART regulations and public financing mechanisms were analyzed to provide information on the healthcare contexts in the countries. The quality of included studies was assessed using the Integrated Quality Criteria for Review of Multiple Study designs.</p><p><strong>Main results and the role of chance: </strong>Of the 4062 studies identified, 26 studies from 17 countries met the inclusion criteria. There were wide disparities across countries in the direct medical costs paid by patients for ART ranging from USD2109 to USD18 592. Relative ART costs and GDP per capita showed a negative correlation, with the costs in Africa and South-East Asia being on average up to 200% of the GDP per capita. Lower relative costs in the Americas and the Eastern Mediterranean regions were associated with the presence of ART regulations and government financing mechanisms.</p><p><strong>Limitations reasons for caution: </strong>Several included studies were not primarily designed to examine the cost of ART and thus lacked comprehensive details of the costs. However, a sensitivity analysis showed that exclusion of studies with below the minimum quality score did not change the conclusions on the outcome of interest.</p><p><strong>Wider implications of the findings: </strong>Governments in LMICs should devise appropriate ART regulatory policies and implement effective mechanisms for public financing of fertility care to improve equity in access. The findings of this review should inform advocacy for ART regulatory frameworks in LMICs and the integration of infertility treatment as an essential service under universal health coverage.</p><p><strong>Study funding/competing interests: </strong>This work received funding from the UNDP-UNFPA-UNICEF-WHO-World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP), a cosponsored programme executed by the World Health Organization (WHO). The authors declare no competing interests.</p><p><strong>Trial registration number: </strong>This review is registered with PROSPERO, CRD42020199312.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2023 2","pages":"hoad007"},"PeriodicalIF":11.1000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10029849/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoad007","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Study question: What are the direct costs of assisted reproductive technology (ART), and how affordable is it for patients in low- and middle-income countries (LMICS)?
Summary answer: Direct medical costs paid by patients for infertility treatment are significantly higher than annual average income and GDP per capita, pointing to unaffordability and the risk of catastrophic expenditure for those in need.
What is known already: Infertility treatment is largely inaccessible to many people in LMICs. Our analysis shows that no study in LMICs has previously compared ART medical costs across countries in international dollar terms (US$PPP) or correlated the medical costs with economic indicators, financing mechanisms, and policy regulations. Previous systematic reviews on costs have been limited to high-income countries while those in LMICs have only focussed on descriptive analyses of these costs.
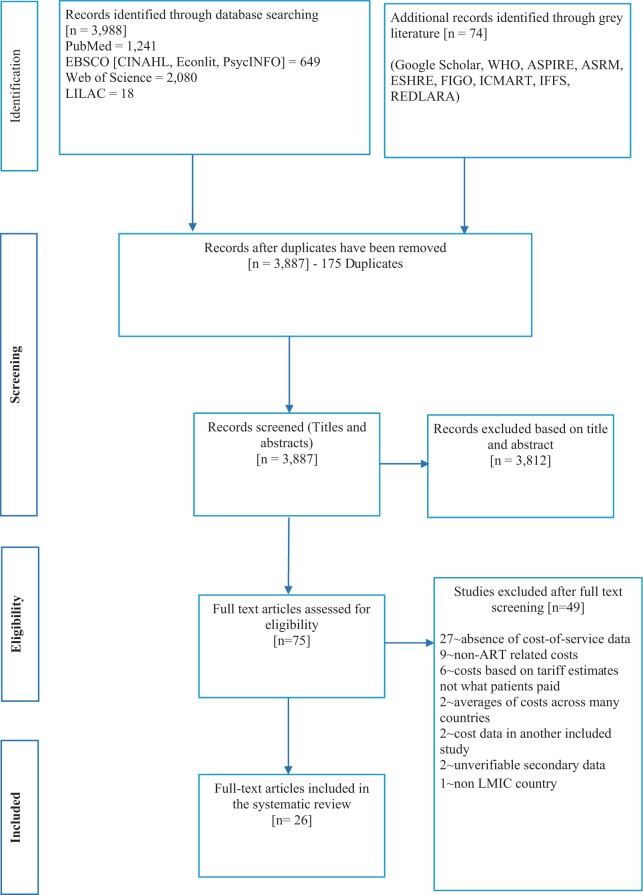
Study design size duration: Guided by the preferred reporting items for systematic reviews and meta-analyses (PRISMA), we searched PubMed, Web of Science, Cumulative Index of Nursing and Allied Health Literature, EconLit, PsycINFO, Latin American & Caribbean Health Sciences Literature, and grey literature for studies published in all languages from LMICs between 2001 and 2020.
Participants/materials setting methods: The primary outcome of interest was direct medical costs paid by patients for one ART cycle. To gauge ART affordability, direct medical costs were correlated with the GDP per capita or average income of respective countries. ART regulations and public financing mechanisms were analyzed to provide information on the healthcare contexts in the countries. The quality of included studies was assessed using the Integrated Quality Criteria for Review of Multiple Study designs.
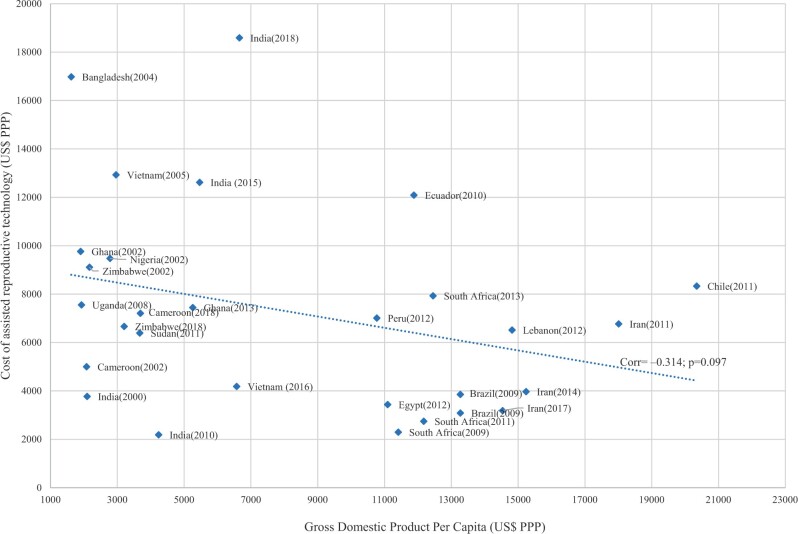
Main results and the role of chance: Of the 4062 studies identified, 26 studies from 17 countries met the inclusion criteria. There were wide disparities across countries in the direct medical costs paid by patients for ART ranging from USD2109 to USD18 592. Relative ART costs and GDP per capita showed a negative correlation, with the costs in Africa and South-East Asia being on average up to 200% of the GDP per capita. Lower relative costs in the Americas and the Eastern Mediterranean regions were associated with the presence of ART regulations and government financing mechanisms.
Limitations reasons for caution: Several included studies were not primarily designed to examine the cost of ART and thus lacked comprehensive details of the costs. However, a sensitivity analysis showed that exclusion of studies with below the minimum quality score did not change the conclusions on the outcome of interest.
Wider implications of the findings: Governments in LMICs should devise appropriate ART regulatory policies and implement effective mechanisms for public financing of fertility care to improve equity in access. The findings of this review should inform advocacy for ART regulatory frameworks in LMICs and the integration of infertility treatment as an essential service under universal health coverage.
Study funding/competing interests: This work received funding from the UNDP-UNFPA-UNICEF-WHO-World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP), a cosponsored programme executed by the World Health Organization (WHO). The authors declare no competing interests.
Trial registration number: This review is registered with PROSPERO, CRD42020199312.
研究问题:辅助生殖技术(ART)的直接成本是多少?低收入和中等收入国家(LMICS)患者的负担能力如何?摘要回答:患者为不孕症治疗支付的直接医疗费用明显高于年平均收入和人均国内生产总值,这表明有需要的人负担不起,而且有灾难性支出的风险。已知情况:低收入和中等收入国家的许多人基本上无法获得不孕症治疗。我们的分析表明,以前没有针对中低收入国家的研究以国际美元(PPP美元)比较各国抗逆转录病毒治疗的医疗费用,或将医疗费用与经济指标、融资机制和政策法规联系起来。以前对成本的系统审查仅限于高收入国家,而中低收入国家的系统审查只侧重于对这些成本的描述性分析。研究设计规模持续时间:在系统评价和荟萃分析(PRISMA)首选报告项目的指导下,我们检索了PubMed、Web of Science、护理和联合健康文献累积指数、EconLit、PsycINFO、拉丁美洲和加勒比健康科学文献,以及2001年至2020年间以所有语言发表的中低收入国家的研究的灰色文献。参与者/材料设置方法:主要研究结果为患者在一个ART周期内支付的直接医疗费用。为了衡量抗逆转录病毒治疗的可负担性,直接医疗费用与各自国家的人均国内生产总值或平均收入相关。分析了抗逆转录病毒治疗条例和公共筹资机制,以提供有关各国卫生保健情况的信息。纳入研究的质量采用多重研究设计评价综合质量标准进行评估。主要结果和偶然性的作用:在4062项研究中,来自17个国家的26项研究符合纳入标准。各国患者为抗逆转录病毒治疗支付的直接医疗费用差异很大,从2109美元到18592美元不等。抗逆转录病毒治疗的相对费用与人均国内生产总值呈负相关,非洲和东南亚的费用平均高达人均国内生产总值的200%。美洲和东地中海区域相对成本较低与抗逆转录病毒治疗法规和政府融资机制的存在有关。注意的局限性:一些纳入的研究的主要目的不是检查抗逆转录病毒治疗的成本,因此缺乏全面的成本细节。然而,敏感性分析表明,排除低于最低质量评分的研究并不会改变对结果感兴趣的结论。研究结果的更广泛影响:中低收入国家政府应制定适当的抗逆转录病毒治疗监管政策,并实施有效的生育护理公共融资机制,以改善获得机会的公平性。这项审查的结果应该为中低收入国家抗逆转录病毒治疗监管框架的宣传提供信息,并将不孕症治疗作为全民健康覆盖下的一项基本服务。研究经费/竞争利益:这项工作得到了开发计划署-人口基金-儿童基金会-卫生组织-世界银行人类生殖研究、发展和研究培训特别方案的经费,这是一个由世界卫生组织(卫生组织)执行的共同赞助方案。作者声明没有利益冲突。试验注册号:本综述注册号为PROSPERO, CRD42020199312。


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
