Catarina Cidade-Rodrigues, Filipe M Cunha, Catarina Elias, Marta Carreira, Isaac Barroso, Paulo Bettencourt, Patrícia Lourenço
{"title":"The prognostic impact of magnesium in acute heart failure is different according to the presence of diabetes mellitus.","authors":"Catarina Cidade-Rodrigues, Filipe M Cunha, Catarina Elias, Marta Carreira, Isaac Barroso, Paulo Bettencourt, Patrícia Lourenço","doi":"10.1097/j.pbj.0000000000000197","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hypermagnesemia predicts mortality in chronic heart failure (HF); however, in acute HF, magnesium does not seem to be outcome-associated. Diabetes mellitus (DM) frequently associates with altered magnesium status. We hypothesized that DM might influence the prognostic impact of magnesium in acute HF.</p><p><strong>Methods: </strong>This is a retrospective cohort study of hospitalized patients with acute HF. Patients without data on admission serum magnesium were excluded. Follow-up: 1 year from hospital admission. Primary end point: all-cause mortality. Patients were divided according to median serum magnesium (1.64 mEq/L). The Kaplan-Meier survival method was used to determine survival curves according to magnesium levels. The analysis was stratified according to the presence of DM. A multivariable Cox regression analysis was used to study the prognostic impact of magnesium.</p><p><strong>Results: </strong>We studied 606 patients. The mean age was 76 ± 12 years, 44.1% were male, 50.7% had DM, and 232 (38.3%) died during follow-up. Median magnesium was 1.64 (1.48-1.79) mEq/L. Patients with magnesium ≥1.64 mEq/L had higher 1-year mortality [141 (46.4%) vs 91 (30.1%), <i>P</i> < .001]. After adjustments for age, sex, history of atrial fibrillation, systolic blood pressure, heart rate, ischemic etiology, B-type natriuretic peptide, estimated glomerular filtration rate, alcohol consumption, antihyperglycaemic agents or glycated hemoglobin, admission glycemia, New York Heart Association class IV, and severe left ventricle systolic dysfunction, serum magnesium ≥1.64 mEq/L was associated with higher mortality only in patients with DM: HR 1.89 (95% confidence interval: 1.19-3.00), <i>P</i> = .007, and 1.27 (95% confidence interval: 0.83-1.94) and <i>P</i> = .26 for non-DM patients. The results were similar if magnesium was analyzed as a continuous variable. Per 0.1 mEq/L increase in magnesium levels, patients with DM had 13% increased risk of 1-year mortality.</p><p><strong>Conclusions: </strong>Higher magnesium levels were associated with worse prognosis only in HF patients with DM.</p>","PeriodicalId":74479,"journal":{"name":"Porto biomedical journal","volume":"7 6","pages":"e197"},"PeriodicalIF":0.0000,"publicationDate":"2022-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a1/9d/pj9-7-e197.PMC10158881.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Porto biomedical journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/j.pbj.0000000000000197","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Hypermagnesemia predicts mortality in chronic heart failure (HF); however, in acute HF, magnesium does not seem to be outcome-associated. Diabetes mellitus (DM) frequently associates with altered magnesium status. We hypothesized that DM might influence the prognostic impact of magnesium in acute HF.
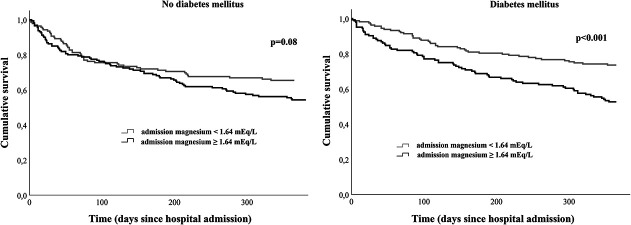
Methods: This is a retrospective cohort study of hospitalized patients with acute HF. Patients without data on admission serum magnesium were excluded. Follow-up: 1 year from hospital admission. Primary end point: all-cause mortality. Patients were divided according to median serum magnesium (1.64 mEq/L). The Kaplan-Meier survival method was used to determine survival curves according to magnesium levels. The analysis was stratified according to the presence of DM. A multivariable Cox regression analysis was used to study the prognostic impact of magnesium.
Results: We studied 606 patients. The mean age was 76 ± 12 years, 44.1% were male, 50.7% had DM, and 232 (38.3%) died during follow-up. Median magnesium was 1.64 (1.48-1.79) mEq/L. Patients with magnesium ≥1.64 mEq/L had higher 1-year mortality [141 (46.4%) vs 91 (30.1%), P < .001]. After adjustments for age, sex, history of atrial fibrillation, systolic blood pressure, heart rate, ischemic etiology, B-type natriuretic peptide, estimated glomerular filtration rate, alcohol consumption, antihyperglycaemic agents or glycated hemoglobin, admission glycemia, New York Heart Association class IV, and severe left ventricle systolic dysfunction, serum magnesium ≥1.64 mEq/L was associated with higher mortality only in patients with DM: HR 1.89 (95% confidence interval: 1.19-3.00), P = .007, and 1.27 (95% confidence interval: 0.83-1.94) and P = .26 for non-DM patients. The results were similar if magnesium was analyzed as a continuous variable. Per 0.1 mEq/L increase in magnesium levels, patients with DM had 13% increased risk of 1-year mortality.
Conclusions: Higher magnesium levels were associated with worse prognosis only in HF patients with DM.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
