Victoria Bünger, Oliver Hunsicker, Alexander Krannich, Felix Balzer, Claudia D Spies, Wolfgang M Kuebler, Steffen Weber-Carstens, Mario Menk, Jan A Graw
{"title":"Potential of cell-free hemoglobin and haptoglobin as prognostic markers in patients with ARDS and treatment with veno-venous ECMO.","authors":"Victoria Bünger, Oliver Hunsicker, Alexander Krannich, Felix Balzer, Claudia D Spies, Wolfgang M Kuebler, Steffen Weber-Carstens, Mario Menk, Jan A Graw","doi":"10.1186/s40560-023-00664-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hemolysis is associated with increased mortality in patients with sepsis, ARDS, or therapy with extracorporeal membrane oxygenation (ECMO). To quantify a critical threshold of hemolysis in patients with ARDS and treatment with veno-venous ECMO, we aimed to identify cutoff values for cell-free hemoglobin (CFH) and haptoglobin (Hp) plasma concentrations associated with a significant increase in ICU mortality.</p><p><strong>Methods: </strong>Patients with ARDS admitted to a tertiary ARDS referral center between 01/2007 and 12/2018 and treatment with veno-venous ECMO were included. Cutoff values for mean CFH (mCFH) and mean Hp (mHp) plasma concentrations dividing the cohort into groups with significantly different ICU mortalities were calculated and patient characteristics were compared. A multiple logistic regression model with stepwise backward variable selection was included. In addition, cutoff values for vulnerable relative timespans for the respective CFH and Hp concentrations were calculated.</p><p><strong>Results: </strong>A quantitative cutoff value of 11 mg/dl for mCFH separated the cohort (n = 442) regarding ICU mortality (mCFH ≤ 11 mg/dl: 38%, [95%-CI: 32.22-43.93] (n = 277) vs. mCFH > 11 mg/dl: 70%, [61.99-76.47] (n = 165), p < 0.001). Analogously, a mHp cutoff value ≤ 0.39 g/l was associated with a significant increase in ICU mortality (mHp ≤ 0.39 g/l: 68.7%, [60.91-75.61] (n = 163) vs. mHp > 0.39 g/l: 38.7%, [33.01-44.72] (n = 279), p < 0.001). The independent association of ICU mortality with CFH and Hp cutoff values was confirmed by logistic regression adjusting for confounders (CFH Grouping: OR 3.77, [2.51-5.72], p < 0.001; Hp Grouping: OR 0.29, [0.19-0.43], p < 0.001). A significant increase in ICU mortality was observed when CFH plasma concentration exceeded the limit of 11 mg/dl on 13.3% of therapy days (≤ 13.3% of days with CFH > 11 mg/dl: 33%; [26.81-40.54] (n = 192) vs. > 13.3% of days with CFH > 11 mg/dl: 62%; [56.05-68.36] (n = 250), p < 0.001). Analogously, a mortality increase was detected when Hp plasma concentration remained ≤ 0.39 g/l for > 18.2% of therapy days (≤ 18.2% days with Hp ≤ 0.39 g/l: 27%; [19.80-35.14] (n = 138) vs. > 18.2% days with Hp ≤ 0.39 g/l: 60%; [54.43-65.70] (n = 304), p < 0.001).</p><p><strong>Conclusions: </strong>Moderate hemolysis with mCFH-levels as low as 11 mg/dl impacts mortality in patients with ARDS and therapy with veno-venous ECMO. Furthermore, a cumulative dose effect should be considered indicated by the relative therapy days with CFH-concentrations > 11 mg/dl. In addition, also Hp plasma concentrations need consideration when the injurious effect of elevated CFH is evaluated.</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"11 1","pages":"15"},"PeriodicalIF":4.7000,"publicationDate":"2023-04-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10116665/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-023-00664-5","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Hemolysis is associated with increased mortality in patients with sepsis, ARDS, or therapy with extracorporeal membrane oxygenation (ECMO). To quantify a critical threshold of hemolysis in patients with ARDS and treatment with veno-venous ECMO, we aimed to identify cutoff values for cell-free hemoglobin (CFH) and haptoglobin (Hp) plasma concentrations associated with a significant increase in ICU mortality.
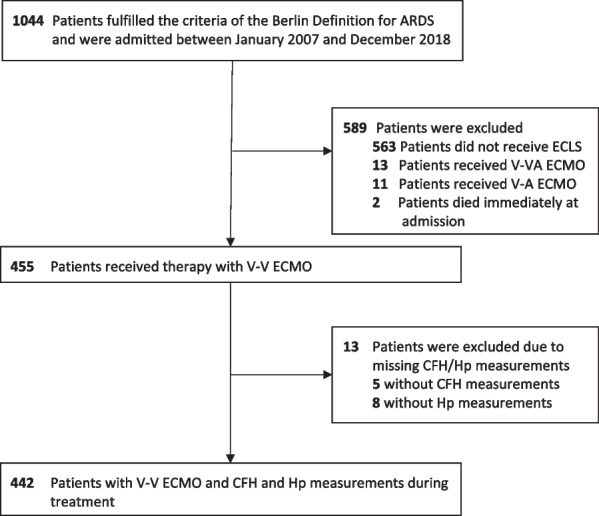
Methods: Patients with ARDS admitted to a tertiary ARDS referral center between 01/2007 and 12/2018 and treatment with veno-venous ECMO were included. Cutoff values for mean CFH (mCFH) and mean Hp (mHp) plasma concentrations dividing the cohort into groups with significantly different ICU mortalities were calculated and patient characteristics were compared. A multiple logistic regression model with stepwise backward variable selection was included. In addition, cutoff values for vulnerable relative timespans for the respective CFH and Hp concentrations were calculated.
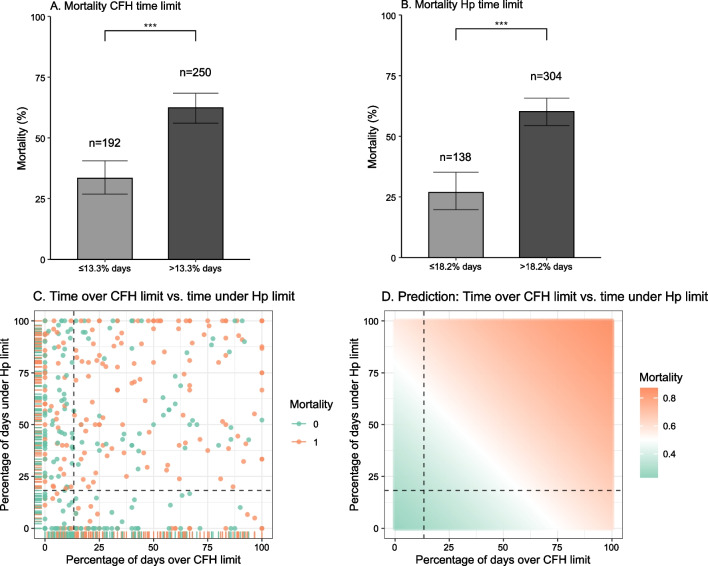
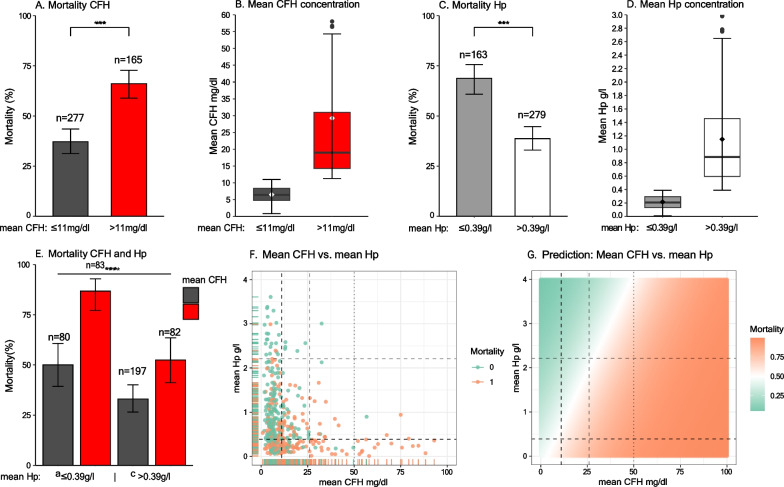
Results: A quantitative cutoff value of 11 mg/dl for mCFH separated the cohort (n = 442) regarding ICU mortality (mCFH ≤ 11 mg/dl: 38%, [95%-CI: 32.22-43.93] (n = 277) vs. mCFH > 11 mg/dl: 70%, [61.99-76.47] (n = 165), p < 0.001). Analogously, a mHp cutoff value ≤ 0.39 g/l was associated with a significant increase in ICU mortality (mHp ≤ 0.39 g/l: 68.7%, [60.91-75.61] (n = 163) vs. mHp > 0.39 g/l: 38.7%, [33.01-44.72] (n = 279), p < 0.001). The independent association of ICU mortality with CFH and Hp cutoff values was confirmed by logistic regression adjusting for confounders (CFH Grouping: OR 3.77, [2.51-5.72], p < 0.001; Hp Grouping: OR 0.29, [0.19-0.43], p < 0.001). A significant increase in ICU mortality was observed when CFH plasma concentration exceeded the limit of 11 mg/dl on 13.3% of therapy days (≤ 13.3% of days with CFH > 11 mg/dl: 33%; [26.81-40.54] (n = 192) vs. > 13.3% of days with CFH > 11 mg/dl: 62%; [56.05-68.36] (n = 250), p < 0.001). Analogously, a mortality increase was detected when Hp plasma concentration remained ≤ 0.39 g/l for > 18.2% of therapy days (≤ 18.2% days with Hp ≤ 0.39 g/l: 27%; [19.80-35.14] (n = 138) vs. > 18.2% days with Hp ≤ 0.39 g/l: 60%; [54.43-65.70] (n = 304), p < 0.001).
Conclusions: Moderate hemolysis with mCFH-levels as low as 11 mg/dl impacts mortality in patients with ARDS and therapy with veno-venous ECMO. Furthermore, a cumulative dose effect should be considered indicated by the relative therapy days with CFH-concentrations > 11 mg/dl. In addition, also Hp plasma concentrations need consideration when the injurious effect of elevated CFH is evaluated.
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
