Comparison of the efficacy and comfort of high-flow nasal cannula with different initial flow settings in patients with acute hypoxemic respiratory failure: a systematic review and network meta-analysis.
{"title":"Comparison of the efficacy and comfort of high-flow nasal cannula with different initial flow settings in patients with acute hypoxemic respiratory failure: a systematic review and network meta-analysis.","authors":"Yuewen He, Xuhui Zhuang, Hao Liu, Wuhua Ma","doi":"10.1186/s40560-023-00667-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>High-flow nasal cannula (HFNC) has been proven effective in improving patients with acute hypoxemic respiratory failure (AHRF), but a discussion of its use for initial flow settings still need to be provided. We aimed to compare the effectiveness and comfort evaluation of HFNC with different initial flow settings in patients with AHRF.</p><p><strong>Methods: </strong>Studies published by October 10, 2022, were searched exhaustively in PubMed, Embase, Web of Science, Cochrane Library (CENTRAL), and the China National Knowledge Infrastructure (CNKI) database. Network meta-analysis (NMA) was performed with STATA 17.0 and R software (version 4.2.1). A Bayesian framework was applied for this NMA. Comparisons of competing models based on the deviance information criterion (DIC) were used to select the best model for NMA. The primary outcome is the intubation at day 28. Secondary outcomes included short-term and long-term mortality, comfort score, length of ICU or hospital stay, and 24-h PaO<sub>2</sub>/FiO<sub>2</sub>.</p><p><strong>Results: </strong>This NMA included 23 randomized controlled trials (RCTs) with 5774 patients. With NIV as the control, the HFNC_high group was significantly associated with lower intubation rates (odds ratio [OR] 0.72 95% credible interval [CrI] 0.56 to 0.93; moderate quality evidence) and short-term mortality (OR 0.81 95% CrI 0.69 to 0.96; moderate quality evidence). Using HFNC_Moderate (Mod) group (mean difference [MD] - 1.98 95% CrI -3.98 to 0.01; very low quality evidence) as a comparator, the HFNC_Low group had a slight advantage in comfort scores but no statistically significant difference. Of all possible interventions, the HFNC_High group had the highest probability of being the best in reducing intubation rates (73.04%), short-term (82.74%) and long-term mortality (67.08%). While surface under the cumulative ranking curve value (SUCRA) indicated that the HFNC_Low group had the highest probability of being the best in terms of comfort scores.</p><p><strong>Conclusions: </strong>The high initial flow settings (50-60 L/min) performed better in decreasing the occurrence of intubation and mortality, albeit with poor comfort scores. Treatment of HFNC for AHRF patients ought to be initiated from moderate flow rates (30-40 L/min), and individualized flow settings can make HFNC more sensible in clinical practice.</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"11 1","pages":"18"},"PeriodicalIF":4.7000,"publicationDate":"2023-05-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10171174/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-023-00667-2","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: High-flow nasal cannula (HFNC) has been proven effective in improving patients with acute hypoxemic respiratory failure (AHRF), but a discussion of its use for initial flow settings still need to be provided. We aimed to compare the effectiveness and comfort evaluation of HFNC with different initial flow settings in patients with AHRF.
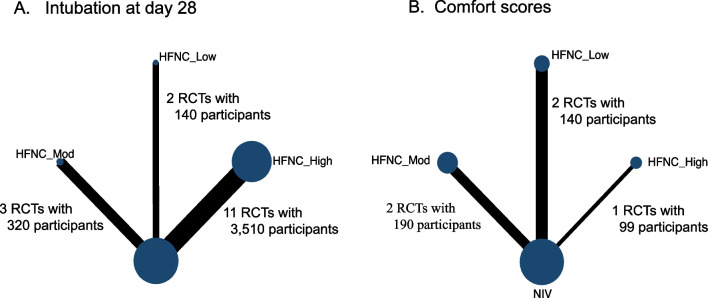
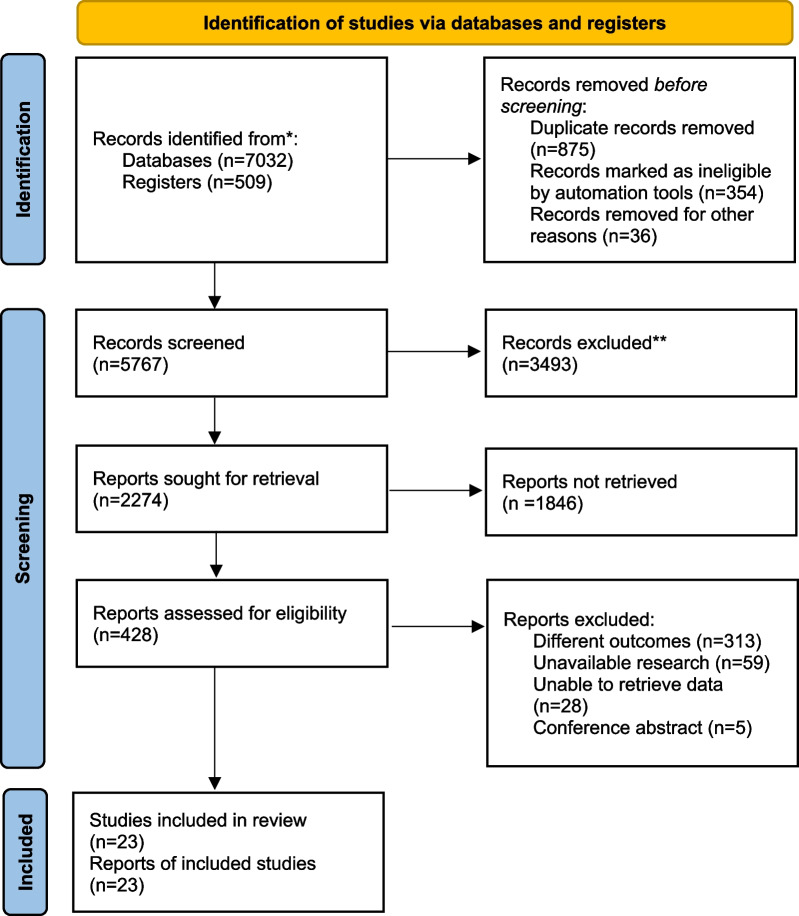
Methods: Studies published by October 10, 2022, were searched exhaustively in PubMed, Embase, Web of Science, Cochrane Library (CENTRAL), and the China National Knowledge Infrastructure (CNKI) database. Network meta-analysis (NMA) was performed with STATA 17.0 and R software (version 4.2.1). A Bayesian framework was applied for this NMA. Comparisons of competing models based on the deviance information criterion (DIC) were used to select the best model for NMA. The primary outcome is the intubation at day 28. Secondary outcomes included short-term and long-term mortality, comfort score, length of ICU or hospital stay, and 24-h PaO2/FiO2.
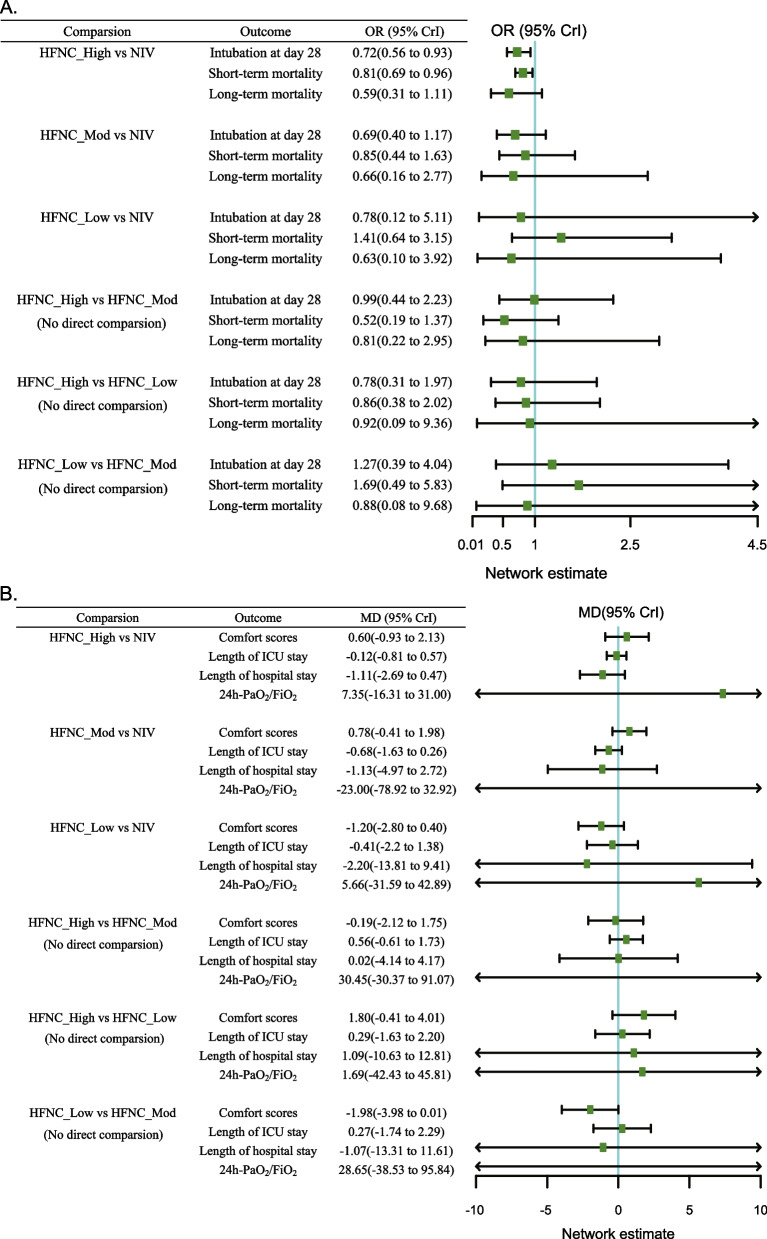
Results: This NMA included 23 randomized controlled trials (RCTs) with 5774 patients. With NIV as the control, the HFNC_high group was significantly associated with lower intubation rates (odds ratio [OR] 0.72 95% credible interval [CrI] 0.56 to 0.93; moderate quality evidence) and short-term mortality (OR 0.81 95% CrI 0.69 to 0.96; moderate quality evidence). Using HFNC_Moderate (Mod) group (mean difference [MD] - 1.98 95% CrI -3.98 to 0.01; very low quality evidence) as a comparator, the HFNC_Low group had a slight advantage in comfort scores but no statistically significant difference. Of all possible interventions, the HFNC_High group had the highest probability of being the best in reducing intubation rates (73.04%), short-term (82.74%) and long-term mortality (67.08%). While surface under the cumulative ranking curve value (SUCRA) indicated that the HFNC_Low group had the highest probability of being the best in terms of comfort scores.
Conclusions: The high initial flow settings (50-60 L/min) performed better in decreasing the occurrence of intubation and mortality, albeit with poor comfort scores. Treatment of HFNC for AHRF patients ought to be initiated from moderate flow rates (30-40 L/min), and individualized flow settings can make HFNC more sensible in clinical practice.
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
