{"title":"Catastrophic Propeller Brain Injury with Large Scalp Defect Treated with Omental Flap.","authors":"Fumihiro Sago, Yusuke Sakamoto, Kenko Maeda, Masaya Takemoto, Jungsu Choo, Mizuka Ikezawa, Ohju Fujita, Daiki Somiya, Akira Ikeda","doi":"10.2176/jns-nmc.2022-0321","DOIUrl":null,"url":null,"abstract":"<p><p>In this study, we report a case of catastrophic propeller brain injury with large scalp defect treated with omental flap reconstruction. A 62-year-old man was accidentally caught in a powered paraglider propeller during maintenance. The rotor blades impacted the left part of his head. On arrival at the hospital, he presented with a Glasgow Coma Scale score of E4V1M4. On some areas on his head, skin was noticeably cut off, and the brain tissue out-slipped through an open skull fracture. Continuous bleeding from the superior sagittal sinus (SSS) and the brain surface was observed during emergency surgery. Massive bleeding from the SSS was controlled using a number of tenting sutures and hemostatic agents. We evacuated the crushed brain tissue and coagulated the severed middle cerebral arteries. Dural plasty using the deep fascia of the thigh was performed. The skin defect was closed using an artificial dermis. The administration of high-dose antibiotics has failed to prevent meningitis. Moreover, the severed skin edges and fasciae were necrotic. Plastic surgeons performed debridement and vacuum-assisted closure therapy to promote wound healing. Follow-up head computed tomography revealed hydrocephalus. Lumbar drainage was performed; however, sinking skin flap syndrome was observed. After removing the lumbar drainage, cerebrospinal fluid leakage occurred. We then performed cranioplasty with a titanium mesh and omental flap on day 31. After the surgery, perfect wound healing and infection control were achieved; however, severe disturbance of consciousness remained. The patient was transferred to a nursing home. Primary hemostasis and infection control are mandatory. An omental flap has been determined to be effective in controlling infection by covering the exposed brain tissue.</p>","PeriodicalId":19260,"journal":{"name":"NMC Case Report Journal","volume":"10 ","pages":"103-108"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/31/e2/2188-4226-10-0103.PMC10185356.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"NMC Case Report Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2176/jns-nmc.2022-0321","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
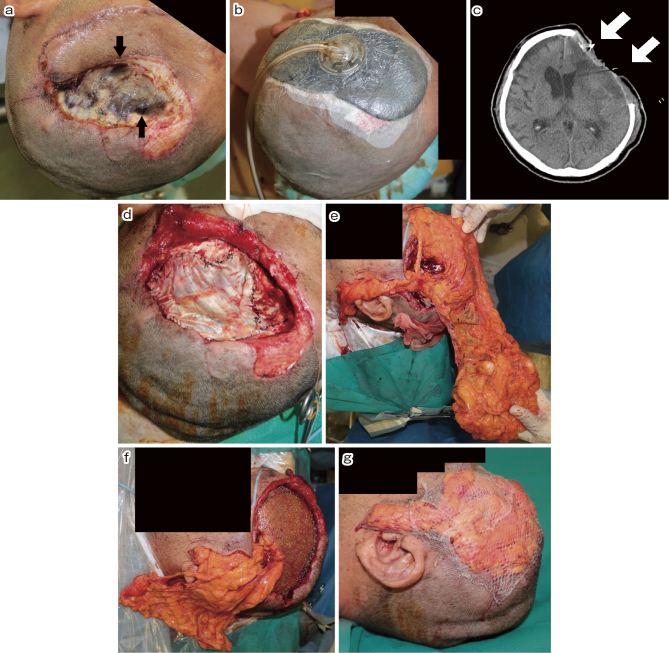
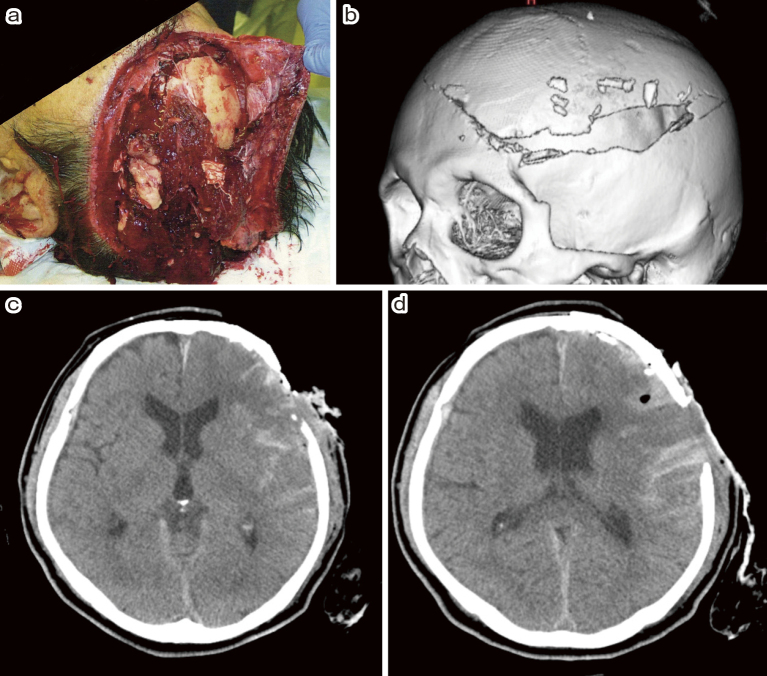
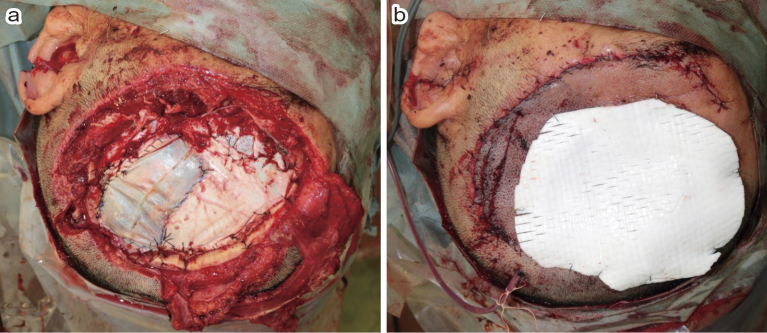
In this study, we report a case of catastrophic propeller brain injury with large scalp defect treated with omental flap reconstruction. A 62-year-old man was accidentally caught in a powered paraglider propeller during maintenance. The rotor blades impacted the left part of his head. On arrival at the hospital, he presented with a Glasgow Coma Scale score of E4V1M4. On some areas on his head, skin was noticeably cut off, and the brain tissue out-slipped through an open skull fracture. Continuous bleeding from the superior sagittal sinus (SSS) and the brain surface was observed during emergency surgery. Massive bleeding from the SSS was controlled using a number of tenting sutures and hemostatic agents. We evacuated the crushed brain tissue and coagulated the severed middle cerebral arteries. Dural plasty using the deep fascia of the thigh was performed. The skin defect was closed using an artificial dermis. The administration of high-dose antibiotics has failed to prevent meningitis. Moreover, the severed skin edges and fasciae were necrotic. Plastic surgeons performed debridement and vacuum-assisted closure therapy to promote wound healing. Follow-up head computed tomography revealed hydrocephalus. Lumbar drainage was performed; however, sinking skin flap syndrome was observed. After removing the lumbar drainage, cerebrospinal fluid leakage occurred. We then performed cranioplasty with a titanium mesh and omental flap on day 31. After the surgery, perfect wound healing and infection control were achieved; however, severe disturbance of consciousness remained. The patient was transferred to a nursing home. Primary hemostasis and infection control are mandatory. An omental flap has been determined to be effective in controlling infection by covering the exposed brain tissue.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
